
The impact of middle hepatic vein reconstruction in right lobe living donor liver transplantation, analysis of congestion area of anterior section and portal vein flow volume
Yoshihiro Hirata1, Shaleen Agarwal1, Subhash Gupta1.
1Centre for Liver and Biliary Science, Max Super Speciality Hospital, Saket, New Delhi, India
Introduction: Middle hepatic vein (MHV) reconstruction in right lobe is reported to contribute better outcome. Large congestion of anterior section in right lobe graft can be a potential cause of small for size syndrome (SFSS), and releasing this congestion with MHV reconstruction would improve the outcome. Another cause of SFSS is high flow volume of portal vein. Portal vein flow volume (PVFV) over 300 ml/min/100g graft weight (GW) was reported as a cause of SFSS. We report how the MHV reconstruction in right lobe graft contribute to better outcome by analyzing congestion area and portal vein flow volume.
Material and method: From February 2017 to December 2018, we had 268 right lobe living donor liver transplantation with MHV reconstruction. MHV was reconstructed with autologous portal vein and consecutive umbilical vein. We classified patients into 4 groups according to PVFV per 100g graft weight, and congestion area ratio (CAR). Group 1 is PFFV < 300ml/m/100g GW, and CAR < 40%, including 83 patients. Group 2 is PF > 300ml/m/100g, and CAR > 40%, including 76 patients. Group 3 is PF < 300ml/m/100g, and CAR < 40%, including 63 patients. Group 4 is PF <300ml/m/100g, and CR <40%, and including 46 patients.
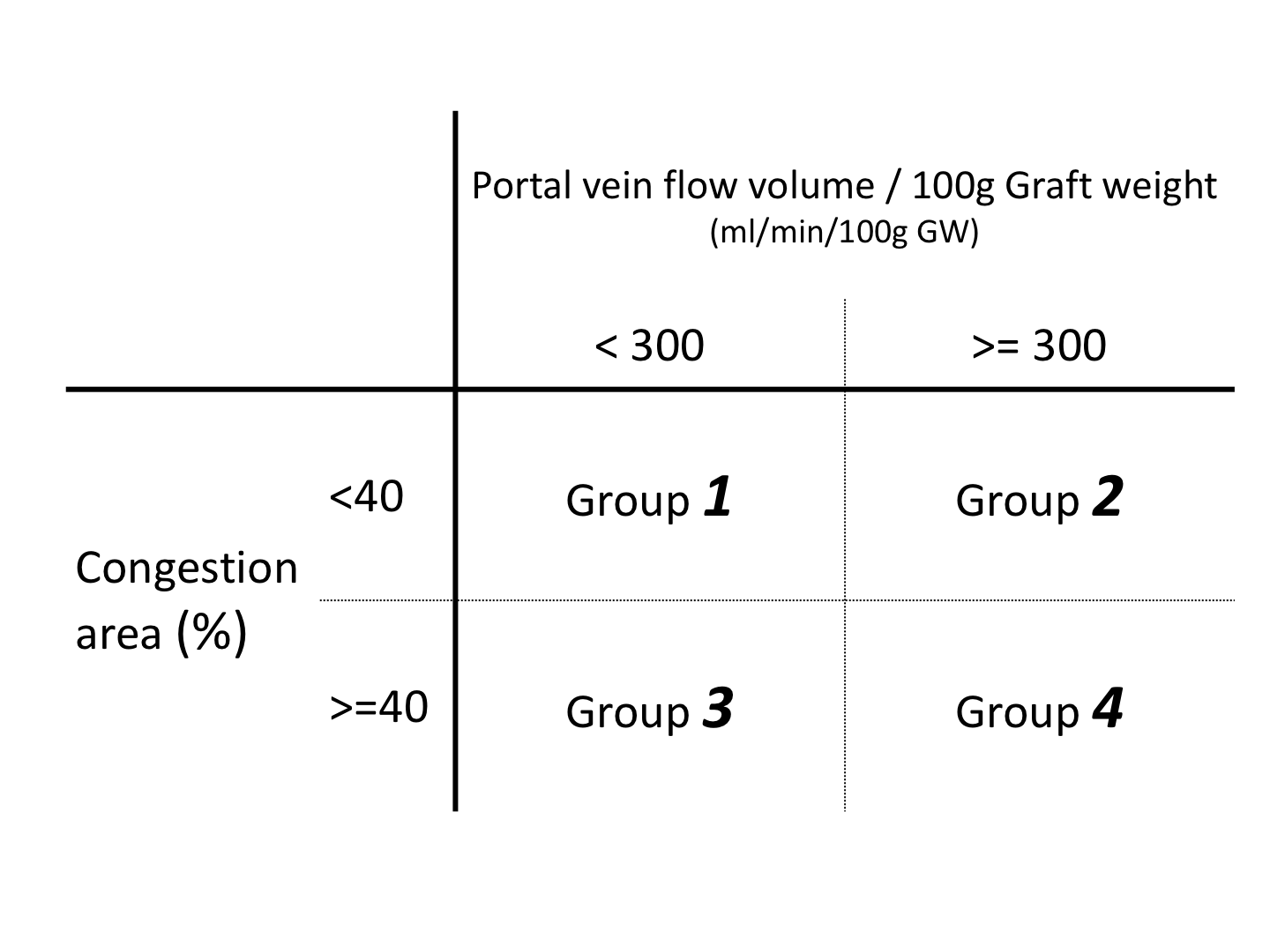
As for Small for size syndrome (SFSS), group 1 is considered as low risk, group 2 and 3 are considered as medium risk, and group 4 patients are considered as high risk. We compared patients background, intraoperative data, and postoperative outcome (postoperative complications, SFSS, and survival) among these 4 groups.
Results: There was no significant difference in preoperative status among 4 groups. Except for congestion area and portal flow volume, there was no significant difference in intraoperative data. There was no significant difference in postoperative complications, incidence of SFSS. The 2 year survival of each group showed no significant difference among 4 groups.
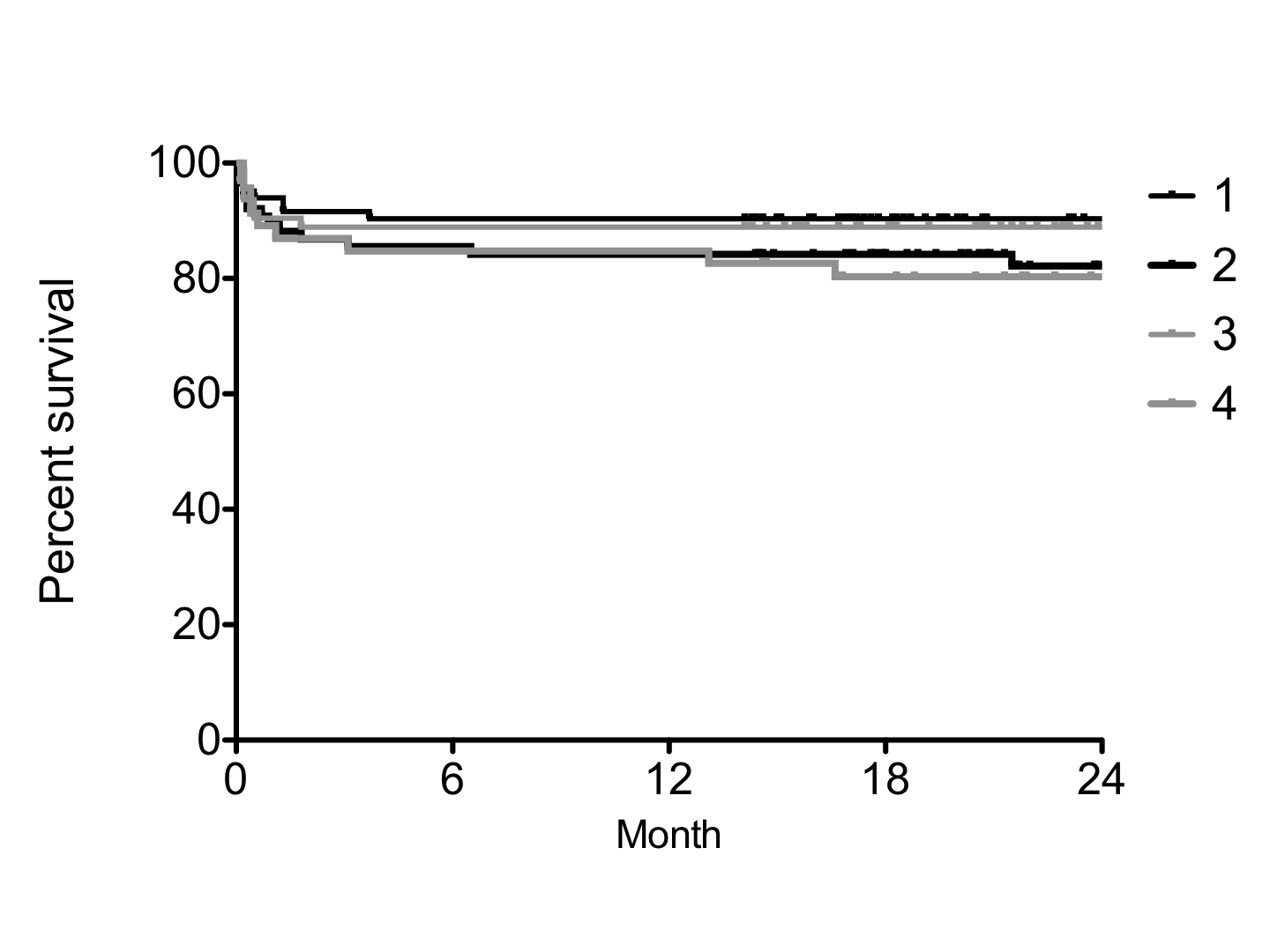
Conclusion: The outcome of medium and high risk groups was equivalent to low risk group. MHV reconstruction release the congestion of anterior section and it also makes tolerate the high portal flow. These factors is considered to make the outcome of medium and high risk group comparable to that of low risk group, and finally the outcome of right lobe living donor liver transplantation result in better outcome.
There are no comments yet...