
The incidence of glucose impairment and new onset diabetes (NODAT) after renal transplant: A retrospective 12-month review at a single UK-centre.
Sameh Mayaleh1, Lauren Quinn1, John Black 1, Islam Eldiasty1, Anna Rizzello1, Tahir Doughman1, Mohamed Morsy1, Atul Bagul1.
1Department of Renal Transplantation & Vascular Access , Leicester General Hospital, Leicester, United Kingdom
Aims: Following Renal transplant, recipients receive a combination of immunosuppressive prophylaxis depending on centre protocol. Whilst these drugs are vital for graft survival, a well-recognised side effect is serum glucose impairment and subsequent new onset diabetes after renal transplantation (NODAT).
Methods: Retrospective data was collected and analysed from 110 patients, who underwent a cadaveric or live renal transplant between January 2018 – December 2018. Electronic records were accessed to decipher recipient blood glucose sugars and HbA1C levels at 1 month, 6 months and 12 months post renal transplant. This data was then utilised to establish the rate of glucose impairment and NODAT incidence at these time intervals.
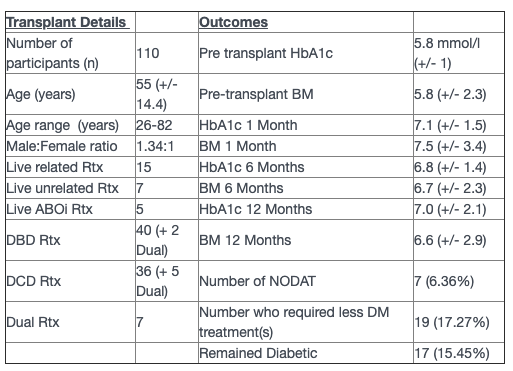
Results: Salient study findings are summarised in the table below. Mean (+/- standard deviations) are used unless otherwise specified.
Discussion: Total number of renal transplants was 110. The unit has a standard immunosuppressive protocol of simulect 20 mg (day 0,4), Methylprednisolone 500 mg at induction. Maintenance includes Mycophenolate mofetil (500mg BD), and Tacrolimus (Trough levels 6-8) and prednisolone 5mg.
The highest average glucose impairment was observed at 1 month following transplant.17 (15.45%) recipients remained diabetic, 67 (60.91%) recipients remained non-diabetic, whilst 7 (6.36%) recipients developed NODAT.
Conclusion: Glucose impairment is seen more commonly within the first 6 months of renal transplant, with a NODAT rate of 6.3% per annum. Interestingly, 19 of 110 recipients (17.2%) who were diabetic pre-transplant showed improved glucose metabolism, and consequently required a reduced diabetic treatment regimen. The maintenance dose of steroids seems to have no impact on NODAT rate. Additionally, post-operative care may be enhanced with diabetologist specialist input for managing glucose impairment and NODAT.
There are no comments yet...