
Milligram to milligram conversion of twice daily to once daily tacrolimus provides equivalent drug exposure in adult kidney transplant
Kanitha Tiankanon1, Natavudh Townamchai1, Stephen Kerr2, Siriwan Thongthip3, Suwasin Udomkarnjananun1, Kriang Tungsanga1, Yingyos Avihingsanon1, Somchai Eiam-Ong1, Kearkiat Praditpornsipa1.
1Division of Nephrology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 2Biostatistics Excellence Centre, Faculty of Medicine. Chulalongkorn University, Bangkok, Thailand; 3Maha Chakri Sirindhorn Clinical Research Center Under the Royal Patronage, Chulalongkorn University, Bangkok, Thailand
Background: Tacrolimus (TAC) is the main immunosuppressive drug for preventing rejection in kidney transplantation. Two oral dose forms are available: Prograf®, a twice daily (BID) Tacrolimus, and Advagraf®, a prolonged released once daily (OD) TAC. OD dosing improves patients’ compliance. Both formulas have comparable efficacy in preventing rejection and similar adverse event rates. Recommended therapeutic trough level (Ctrough) of OD TAC is controversial. When conversion of BID TAC to OD TAC at the same total daily dose, Ctrough level significantly decreases below the recommended level for BID Tac. Therefore, physician tends to increase the total daily dose.
Objective: To compared the AUC at 24 hours (AUC0-24h) and Ctrough between OD TAC and BID TAC.
Methods: A single center, open-labeled pharmacokinetic (PK) study was conducted at King Chulalongkorn memorial hospital. Kidney transplant patients with age ≥18 years, stable kidney function (baseline serum creatinine < 3.0 mg/dL), and duration after transplantation > 6 months were enrolled. Conversion from BID TAC to OD TAC at ratio of 1:1 mg was performed. AUC0-24h, Ctrough, peak concentration (Cmax), time to Cmax (Tmax), and half-life were assessed at 4 weeks after drug switching. A 90% confidence interval of geometric mean ratio (GMR) within range of 0.9 – 1.10 would determine equivalent drug exposure.
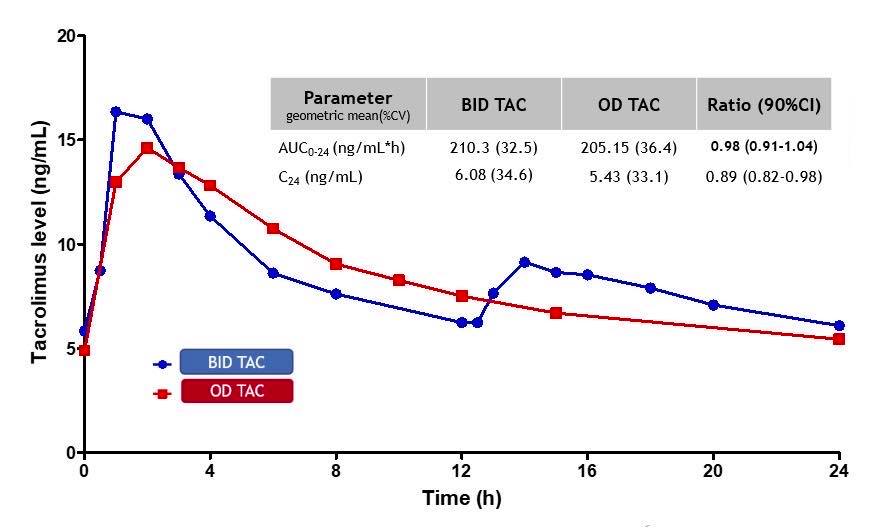
Results: Twenty patients (60% males, aged 26-64 years) were enrolled. Median time since transplantation was 18 months. Baseline serum creatinine was 1.34 (±0.32) mg/dL. Mean total daily TAC dose was 0.073 (±0.05) mg. The geometric mean (%CV) of AUC0-24h of BID and OD TAC were 210.3 (32.5) and 205.15 (36.4) ng/mL*h respectively. There was a stronger correlation between Ctrough and AUC0-24h of OD than BID TAC (R2 = 0.80 VS 0.71). While Ctrough was significantly lower with OD TAC (GMR = 0.89 (90%CI 0.82-0.98)), the AUC0-24h was not different (GMR = 0.98 (90%CI 0.91-1.04). The eGFR and biopsy proven rejection at 1 and 3 month of OD TAC was not increased.
Conclusion: Conversion from BID to OD TAC with equivalent daily dose is appropriate with similar immune functions and graft outcomes. Despite the 11% decrease in Ctrough of OD TAC, increasing dose is not necessary.
There are no comments yet...