
H1N1: A forgotten and mysterious entity in post renal transplant patients
Sanshriti Chauhan1, Vivek Kute1, Himanshu Patel1, Divyesh Engineer1, Sudeep Desai1.
1Nephrology, IKDRC-ITS, Ahmedabad, India
Introduction: H1N1 can present with mild flu like illness to severe respiratory failure and death. But H1N1 presentation and course in renal transplant is still an enigma. There were few case reports in past pandemics. There has not been any published data in renal transplant patients in 2017-2019. We attempt to address few questions like the severity of infection, predictors of mortality, utility of vaccine, prophylaxis, and treatment protocol in patients affected with H1N1.
Methods: All the renal transplant patients with suspected H1N1 were admitted and all routine laboratory samples were sent. Cases were defined as suspected, probable, or confirmed according to diagnostic method. Treatment comprised of oseltamavir for 5 days, and symptomatic care. Immunosuppression were curtailed according to severity of infection.
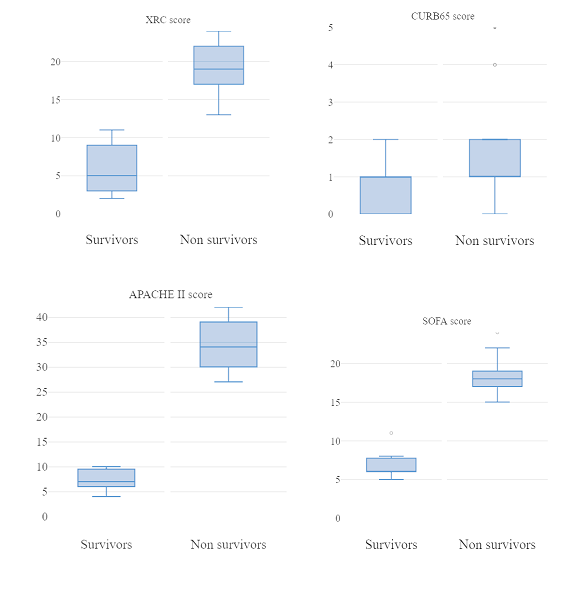
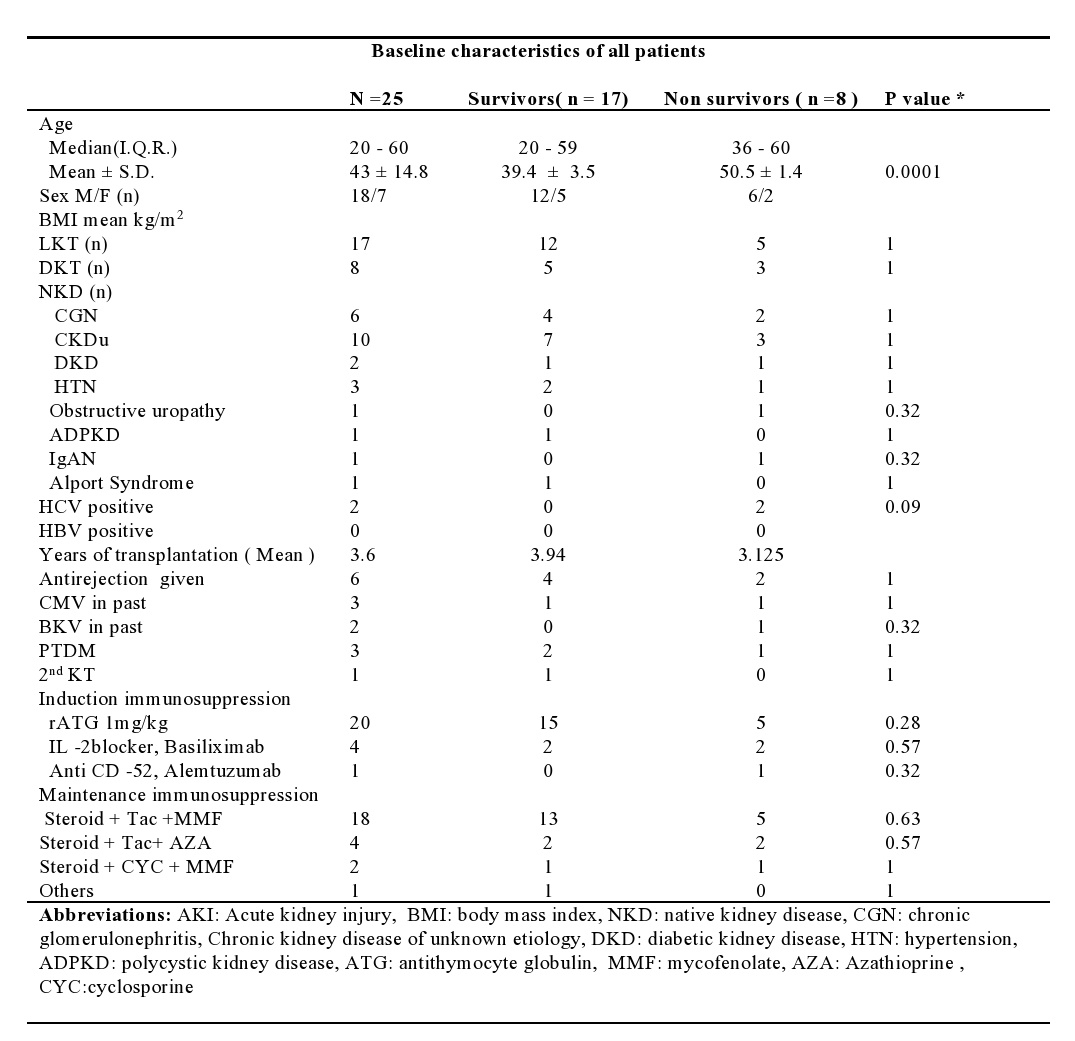
Results: We report 40 cases of H1N1 in renal transplants. Then mean age of presentation was 43 ± 14.8 (20- 60) with males getting more affected. There was an extreme statistical difference among group of non survivors and survivors. Number of patients in DKT and LKT were 8 and 17 and there was no statistical difference in terms of outcome. 14 cases in the year 2017, 7 cases in 2018 and 4 cases were detected in the calendar 2019 respectively. Most cases were from September, October and January in 2017, 2018, and 2019 respectively. 3/14, 3/7, and 1/4 case died in 2017, 2018 and 2019 respectively. 14(56%) patients maintained saturation in room air and had a mild course. 9(35%) required intubation and mechanical ventilation and 2 recovered from supplemental O2. Only 1 of the 9 ventilated patients was able to recover from illness. 10 (36%) patients developed AKI of which only 1 survived. Interestingly neither initial symptoms nor CURB65score predicted mortality, but high APACHEII, SOFA scores predicted mortality.
Discussion: H1N1 has shown wide diversity in severity and seasonality over the decade. India, previously reported peak cases were in Jan-March, now it is reversed to Aug-Oct, which corresponds to our study. Out of 40 confirmed cases, 80% were asymptomatic, there would be more possible asymptomatic H1N1 recipients in community which were never screened, so the exact burden of H1N1 in renal transplants stays undetermined. Gooskens J et al has shown that drugs were effective even when started which is contrary to us. Helentra et al showed more severe cases where timing of diagnosis of H1N1 infection and transplant was short this is in contrast to our study. Surprisingly we never had a single case of H1N1 in their first year of transplant. Our study showed we are still are clueless in treating, or even predicting severity in H1N1 infection in post renal transplants.
Conclusion: This study highlights the changing pattern of H1N1, and failure of initial assessment tools to predict mortality. Vaccination and antiviral therapies effectiveness is still questionable.