
Familial amyloid polyneuropathy domino liver transplantation: What did we do right?
Ahmad Karadagi1,2, Viktor Renneus Guthrie1, Felicia Kjaernet1, Antonio Romano1, Bo-Göran Ericzon1,2, Greg Nowak1,2.
1PO Transplantation, Karolinska University Hospital, Stockholm, Sweden; 2Department of Clinical Science, Intervention and Technology (CLINTEC), Karolinska Institutet, Stockholm, Sweden
Introduction: Domino liver transplantation (DLT) has been used to lessen organ shortage and expand the pool of organs that can be used for liver transplantation (LT). Familial amyloid polyneuropathy (FAP) is a neurodegenerative disorder caused by transthyretin gene mutation, where the effects of the mutation are strictly extra hepatic. Explanted livers from FAP patients have been used to expand the donor pool. Since symptoms due to the inborn error is not seen until young adulthood, recipients of FAP livers may be free of symptoms up to 20 years after transplantation, therefore patients at our center such as those older than 60 years or with hepatocellular carcinoma were selected for DLT. The aim of the study was to evaluate the effect of domino grafts on waiting list duration and patient survival whether these patients were transplanted with a standard or domino graft.
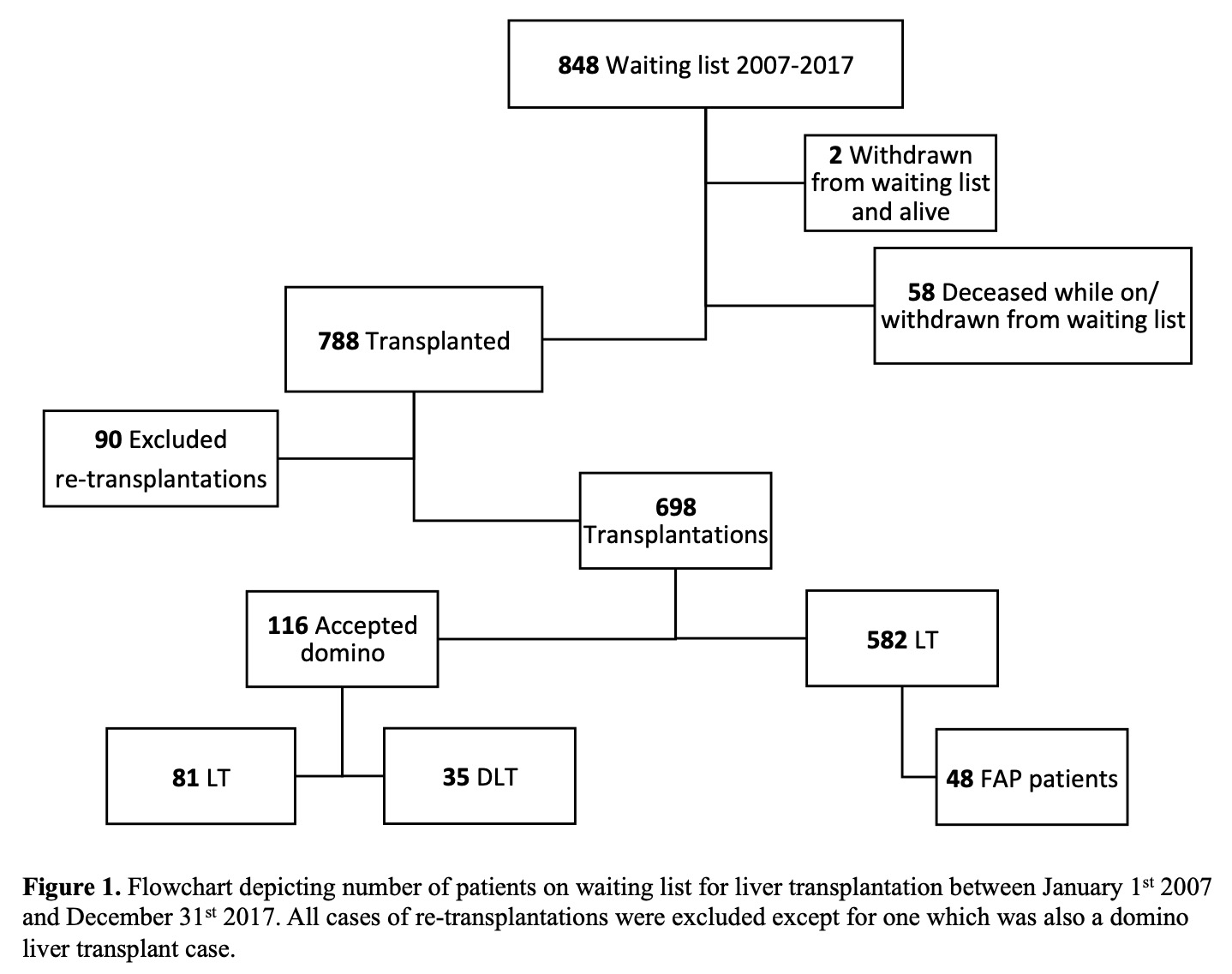
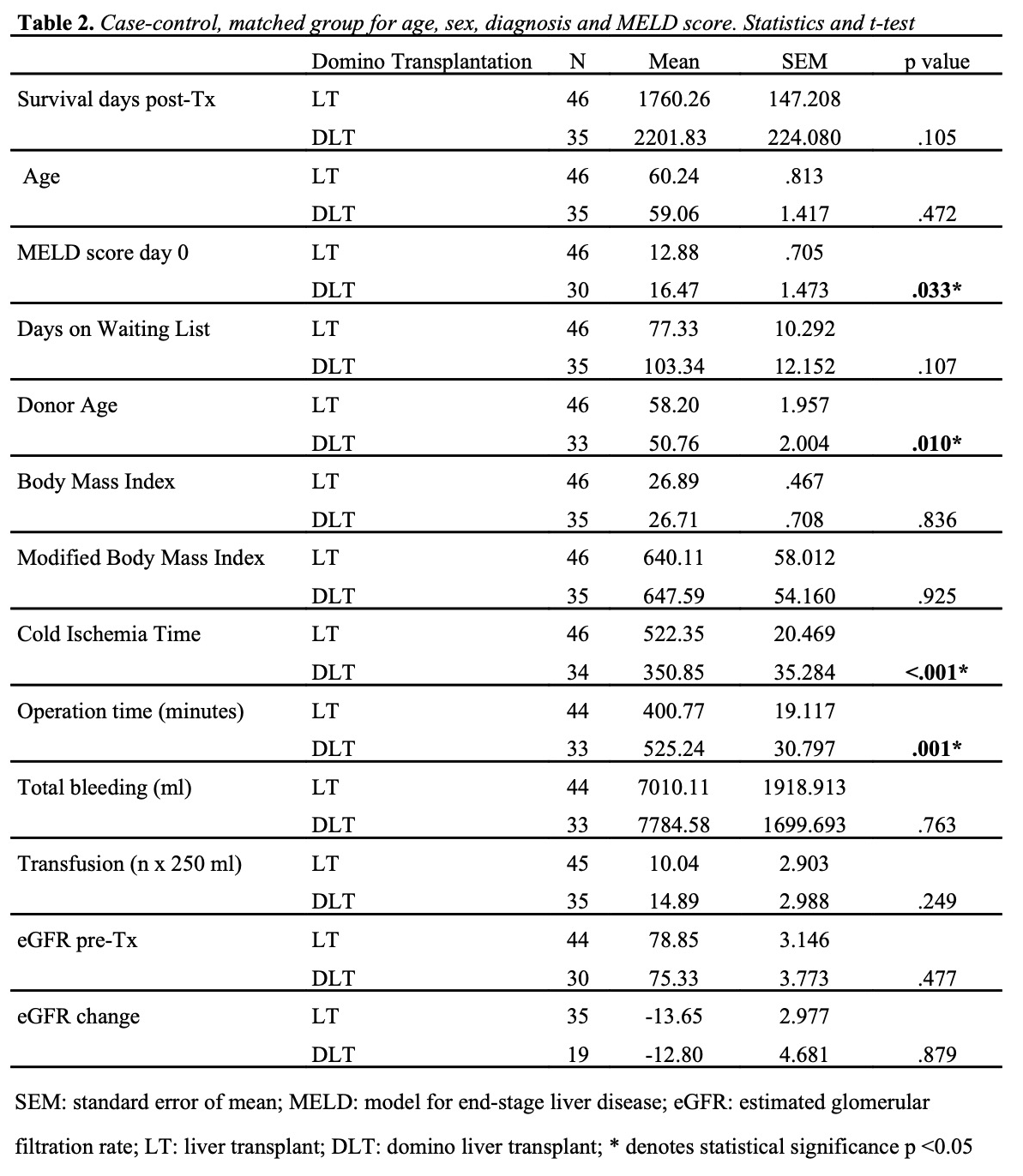
Material and Methods: Patient records and waiting time from all LTs performed at our center between 2007 and 2017 were analyzed in a retrospective cohort study. All cases of re-transplantation were excluded. All domino cases were included regardless of age or re-transplantations. Patients accepting DLT were divided according to whether they went on to receive a standard deceased donor LT or a DLT. Comparisons were made to evaluate survival, waiting time, operative factors and characteristics. To more specifically examine the impact of domino transplantation, a case-control method was used to match for age, sex, diagnosis, and MELD score.
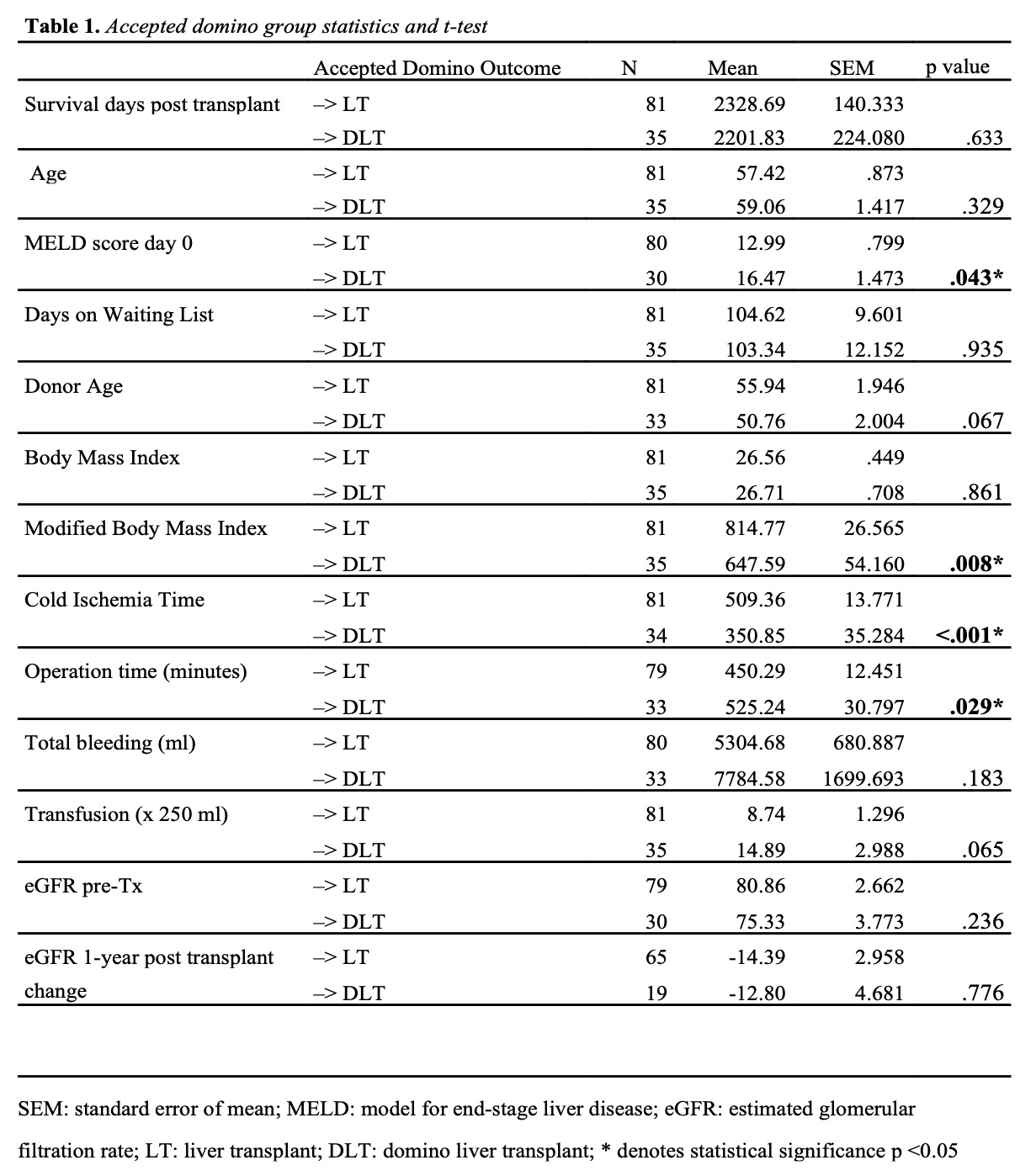
Results: In total 698 transplantation cases were identified, 615 (88.1%) standard LT, 35 (5.0%) DLT and 48 (6.9%) FAP patients. Of the included patients, 116 accepted DLT, of which 81 did receive a standard LT.
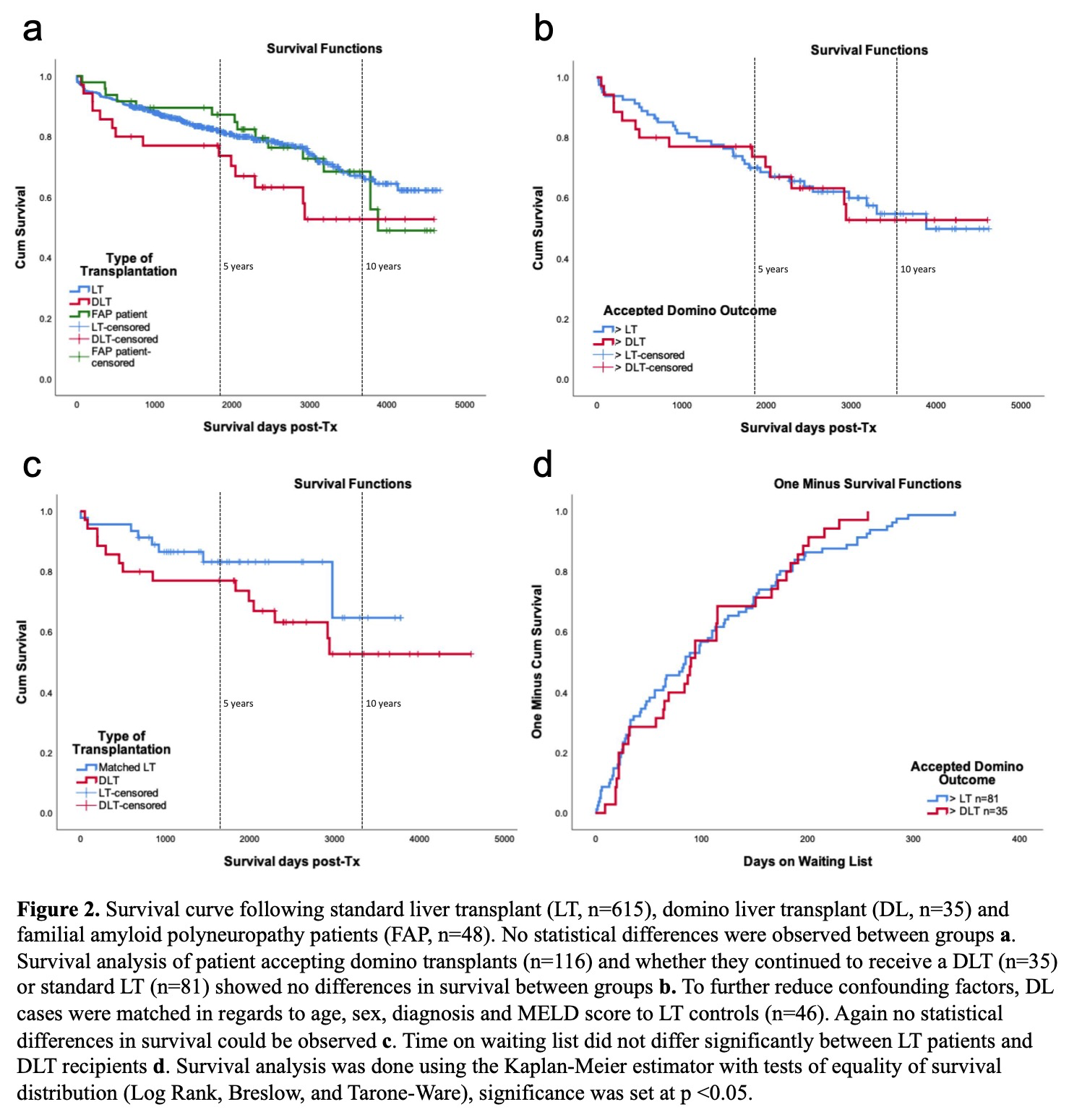
Five-year survival was the same for LT 64.2% and DLT 65.7% within the group accepting domino. However, in the matched case-control group, 5-year survival was for LT 39.1% and DLT 65.7% (Pearson Chi-square, p=0.018), 1 year survival showed no difference. Overall survival estimation was similar within groups, as was waiting time.
As to be expected, cold ischemia time was significantly shorter for the DLT group (351 vs. 509 minutes, t-test, p<.001) and operating time was longer (525 vs. 450, p=.029). MELD score was higher for DLT patients (p=.043 unmatched, p=.33 matched).
Discussion: No major differences were seen between domino and standard LT groups. DLT does not affect the waiting time or survival on an individual basis. Higher MELD score in patients who received a domino graft seem to reflect patients in worse condition being selected for DLT. If matched to similar indications, survival improved after 5 years among patients transplanted with DLT.
Conclusion: Domino transplantation has enabled the transplantation of more patients (5% more liver grafts), many of whom may not have been transplanted otherwise but does not reduce waiting time on an individual level.
[1] Barreiros AP, Galle PR, Otto G. Familial amyloid polyneuropathy Dig Dis 2013; 31: 170.
[2] Furtado A, Tome L, Oliveira FJ, Furtado E, Viana J, Perdigoto R. Sequential liver transplantation. Transplant Proc 1997; 29: 467.