
Prospective non-randomized open label trial comparing outcome of open versus robotic pediatric kidney transplant at single centre
Dhruv Patel1, Suresh K. Singla1, Amit Mishra1, Rohit Chauhan1, Himanshu Patel3, Vivek Kute3, Anshuman Saha2, Kinnari Vala2, Pranjal Modi1.
1Urology and Transplantation Surgery, Institute of Kidney Diseases and Research Centre, Ahmedabad, India; 2Pediatric Nephrology, Institute of Kidney Diseases and Research Centre, Ahmedabad, India; 3Nephrology, Institute of Kidney Diseases and Research Centre, Ahmedabad, India
Introduction: Kidney transplant is the standard of care in pediatric patients suffering from end stage renal disease (ESRD). Pediatric patients pose difficulty in open kidney transplantation (OKT) due to disproportionately large size of incision as compared to the abdomen, and greater amount of blood loss and post operative pain, hence we propose robotic kidney transplant (RKT) as an effective and less invasive technique with comparable or better results. Here we have compared perioperative and postoperative outcomes of RKT versus OKT in pediatric patients.
Materials and Methods: This was open label prospective non-randomized observational study comparing 60 pediatric patients who underwent RKT and 22 underwent OKT from April 2013 to October 2019 at Institute of kidney diseases and research Centre, Ahmedabad. In RKT, with the use of veress needle pneumoperitoneum was created and ports were placed. Da Vinci Si surgical platform was used for RKT. After dissecting external or common iliac vessels, vascular anastomosis was carried out by Gore tex cv-6 suture. In OKT vascular anastomosis was carried out by prolene 6-0 suture. Ureteric reimplantation was carried out with vicryl 4-0 by modified Lich-Gregoir technique. Postoperatively s.creatinine was monitored on day 1, day 7, 1 month, 6 month and then every 6 monthly. The primary end point of the study was Feasibility of RKT and secondary end point was S.creatinine value at 30 days.The graft and patient survival were calculated using Kaplan meire curve analysis and Log Rank test.
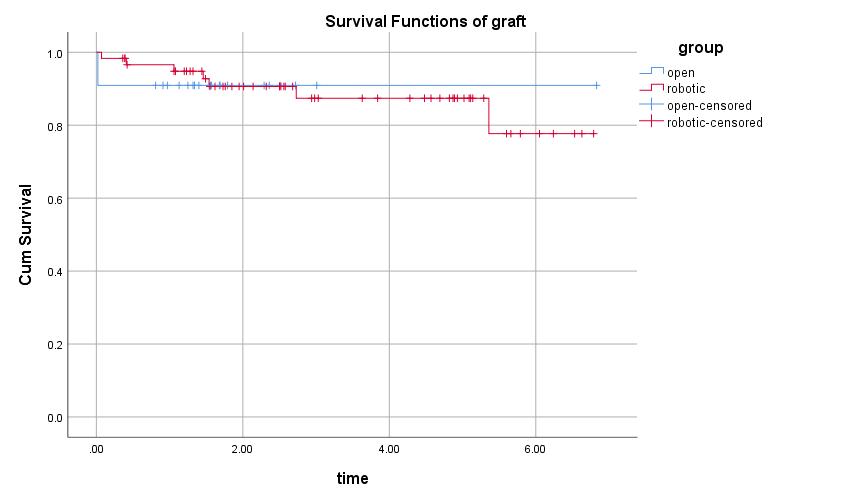
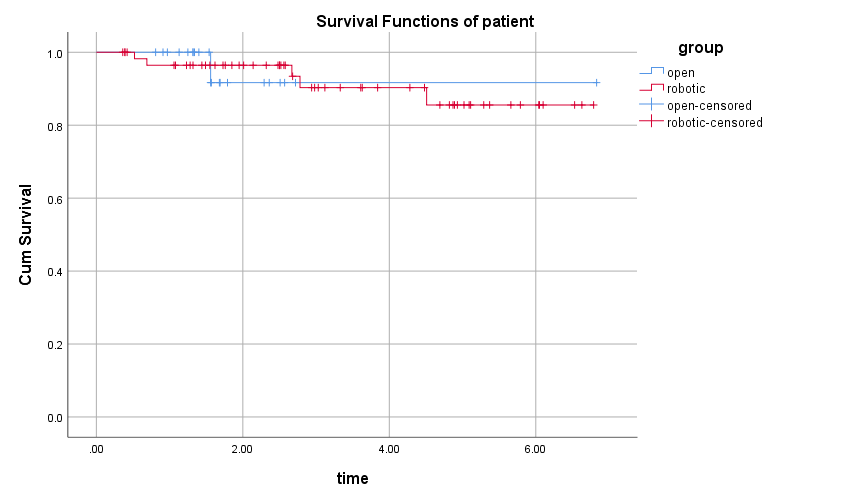
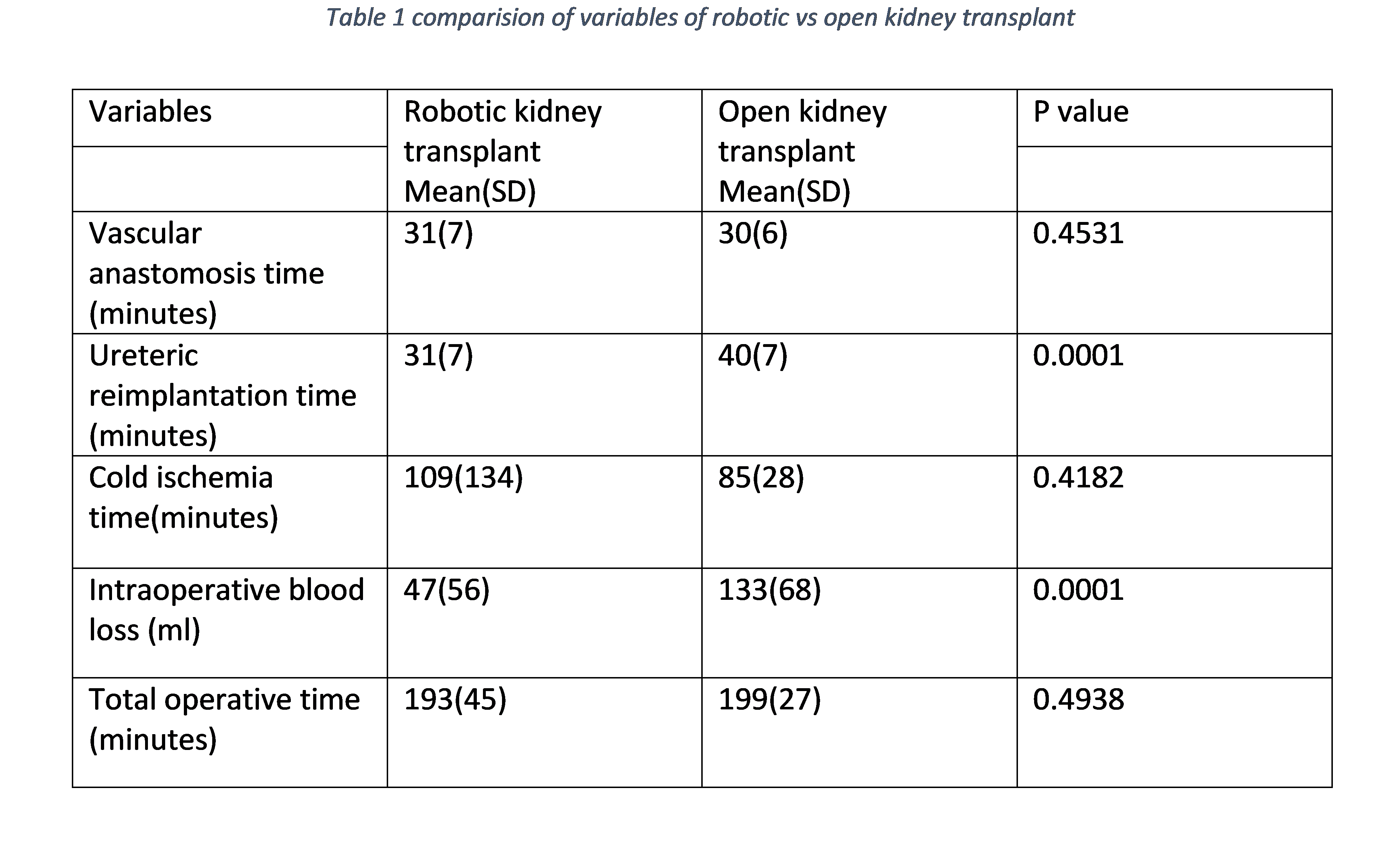
Results and Discussion: Out of 60 pediatric patients underwent RKT, 51 were male and 9 were female.The mean cold ischemia time and rewarming time was 109 (±134) and 44(±10) minutes respectively. Average time taken for vascular anastomosis was 31 (±7) minutes. The mean ureteric reimplantation time was also 31 (±7) minutes. The mean intraoperative blood loss was 47 (±56) ml. Average total console time and total operative time was 131 (±36) and 193 (±45) minutes respectively. 5 patients had slow graft function. During follow up 7 patients lost graft, out of which 2 had acute antibody mediated rejection, 4 had chronic rejection, one had denovo collapsing glomerulopathy with BKV nephropathy. 5 patients expired during follow up.
22 patients operated for OKT out of which 17 were male and 5 were female. Average time for vascular anastomosis and ureteric reimplantation was 30 (±6, p=0.4531) and 40 (±7, p=0.0001) minutes respectively. Mean cold ischemia time was 85 (±28, p=0.4182) minutes. Mean intraoperative blood loss was 133 (±68, p=0.0001) ml. Total operative time was 199 (±27, p=0.4938) minutes. 2 patients had slow graft function. 2 patients lost graft and 2 patients expired during follow up.
There was no statistically significant difference in terms of graft survival and overall patient.
Conclusion: Robotic kidney transplant is technically safe and feasible in pediatric patient suffering from ESRD.