
Panel reactive antibody and the association of early steroid withdrawal with kidney transplant outcomes
Sunjae Bae1,2,3, Mara A. McAdams-DeMarco1,2, Allan B. Massie1,2, Jacqueline M. Garonzik-Wang2, Josef Coresh1,3,4, Dorry L. Segev1,2.
1Epidemiology, Johns Hopkins University, Baltimore, MD, United States; 2Surgery, Johns Hopkins University, Baltimore, MD, United States; 3Biostatistics, Johns Hopkins University, Baltimore, MD, United States; 4Medicine, Johns Hopkins University, Baltimore, MD, United States
Introduction: Early steroid withdrawal (ESW) is a viable maintenance immunosuppression strategy in certain low-risk kidney transplant recipients. A low panel reactive antibody (PRA) may indicate low-risk condition amenable to ESW. We aimed to identify the threshold value of PRA above which ESW may pose additional risk, and to compare the association of ESW with transplant outcomes across PRA strata.
Materials and Methods: Using the US national registry data, we studied 121,699 deceased-donor kidney-only recipients in 2002-2017. Using natural splines and ESW-PRA interaction terms, we explored how the associations of ESW with transplant outcomes change with increasing PRA values, and discovered rapid exacerbation in PRA>60 (Figure 1). Then, we assessed whether PRA>60 modifies the associations of ESW with 1-year acute rejection, death-censored graft failure, and death.
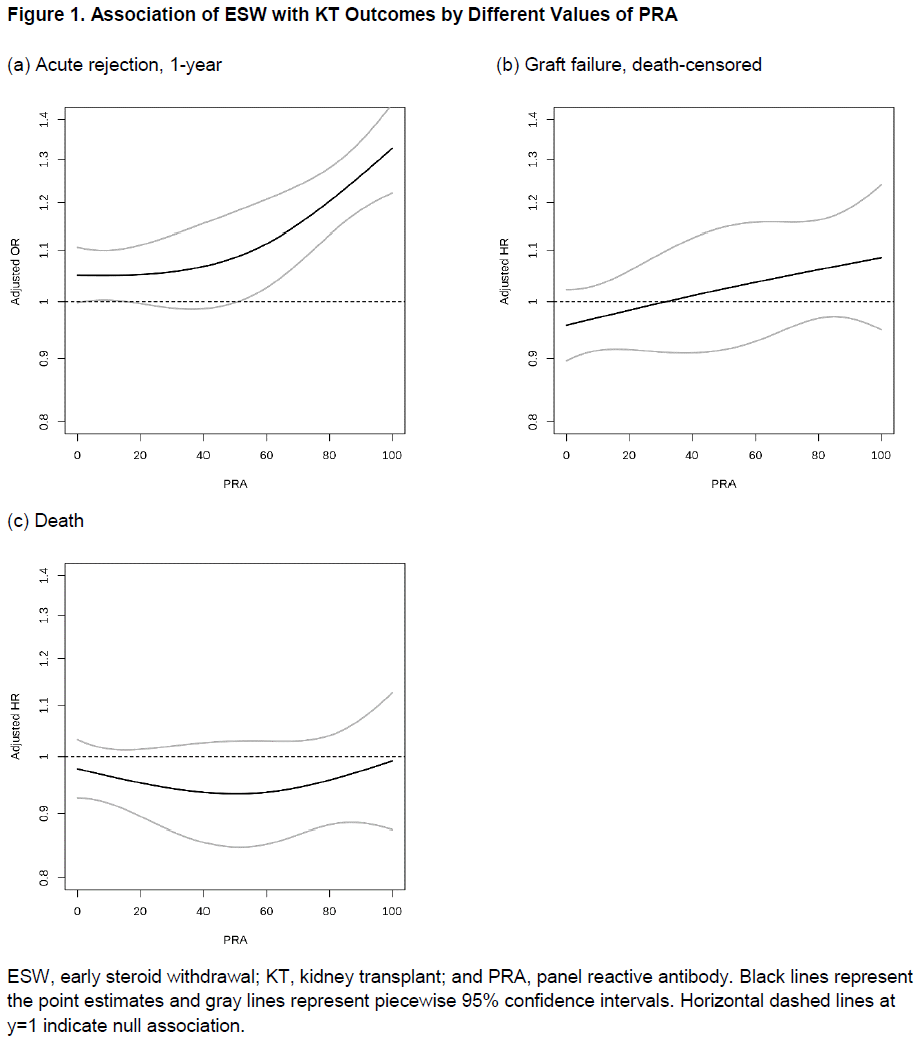
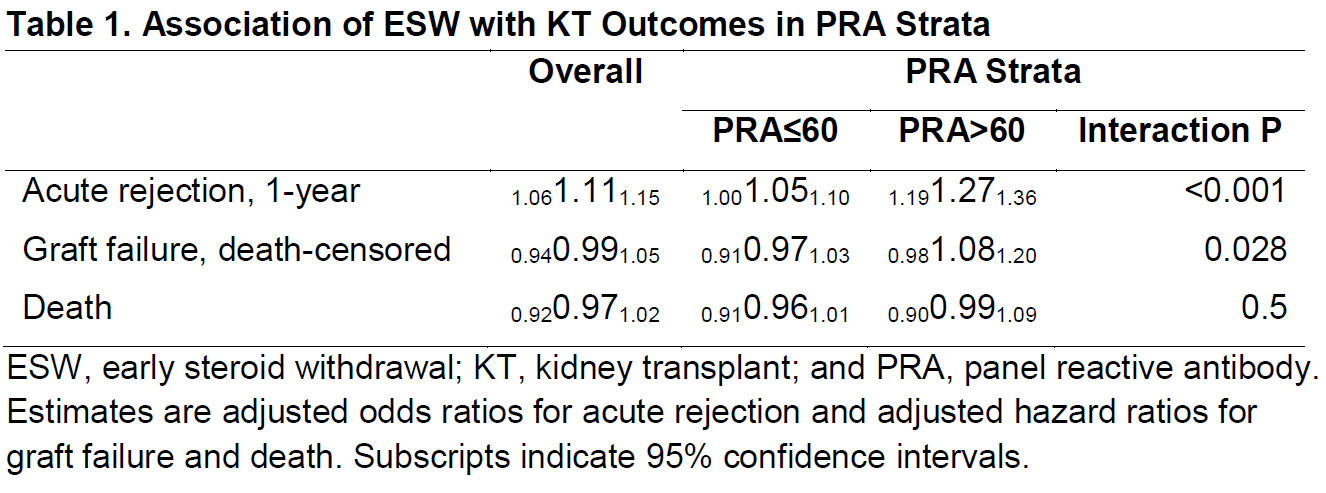
Results: Among PRA≤60 recipients, ESW was associated with a minor increase in rejection (aOR=1.001.051.10) and with a tendency of decreased graft failure (aHR=0.910.971.03; Table 1). However, among PRA>60 recipients, ESW was associated with a substantial increase in rejection (aOR=1.191.271.36; interaction p<0.001) and with a tendency of increased graft failure (aHR=0.981.081.20; interaction p=0.028). The association of ESW with death was similar between PRA strata (PRA≤60, aHR=0.910.961.01; and PRA>60, aHR=0.900.991.09; interaction p=0.5).
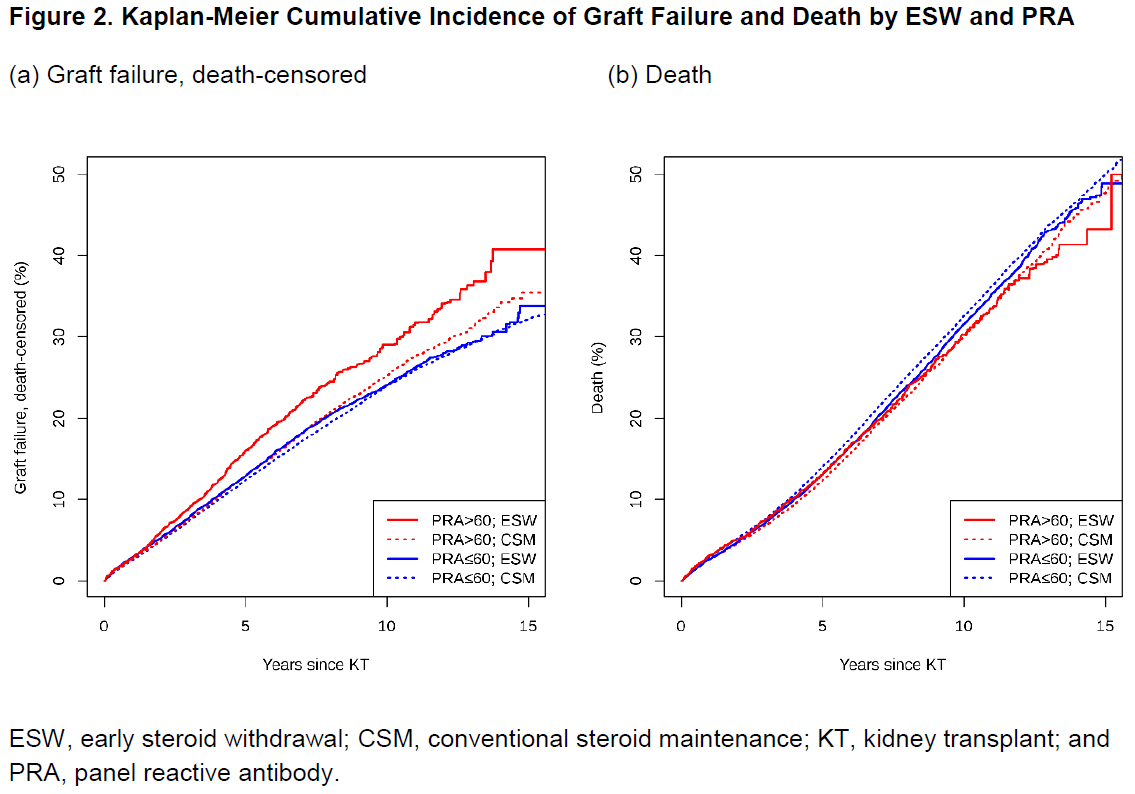
Conclusion: The associations of ESW with rejection and graft failure were significantly more adverse in recipients with high PRA, especially those above 60. PRA should be considered in the risk assessment for ESW tailoring.
American Society of Nephrology. National Institutes of Health.