
Does the cold storage really «cold»? Liver thermography and microdialysis findings
Alexander Sushkov1, Vladimir Rudakov1, Anna Maltseva1, Daria Svetlakova1, Konstantin Gubarev1, Dmitry Zabezhinsky1, Alexey Artemiev1, Sergey Voskanyan1.
1Surgery and Transplantation Center, State Research Center – Burnasyan Federal Medical Biophysical Center (SRC-FMBC), Moscow, Russian Federation
Background: We suggest that in clinical practice organ temperature (Temp) during static cold storage is an underestimated factor affecting both the organ metabolic state before transplantation and the initial graft function. To verify this hypothesis we conducted a pilot clinical study involving living (LD) and deceased donors (DD) liver grafts.
Material and Methods: The study included 4 LD right lobe liver grafts (cases L1 – L4) and 7 grafts from standard criteria DD with brain death (cases D1 – D7). Two DD grafts were not transplanted due to prolonged cold ischemia time (CIT) exceeding 13 hours (cases D6 and D7). Histidine-tryptophan-ketoglutorate solution was used for all grafts.
Thermography (Guide D160) and microdialysis (M Dialysis AB, Sweden) were performed in each case at the end of the CIT. Microdialysis catheter was placed in SIV (for DD) or in SVIII (for LD). Samples of interstitial fluid were collected within 30-45 minutes before thermography and analysed for glucose (Glu), lactate (Lac), pyruvate (Pyr) and glycerol (Glyc).
All transplantations were primary, non-urgent, performed in patients with cirrhosis and MELD value of 12-24 points.Early allograft dysfunction (EAD) was diagnosed with Olthoff criteria. There were no primary non-functioning grafts.
Results and Discussion: CITs for LD grafts were: 0,5 – 1,0 h (median–0,5); for all DD grafts: 8,0 – 14,0 h (median–11,0) and for DD transplanted grafts: 8,0 – 12,5 (median–9).
The medians of Temp [T(med)] were significantly higher than 4°C and varied widely. For LD: 13.4°C - 16.8°C, for DD: 7.7°C - 12.4°C. Moreover, the Temp of each individual graft also varied widely: the difference between the hottest and coldest points was in the range of 3.5°C – 7.3°C.
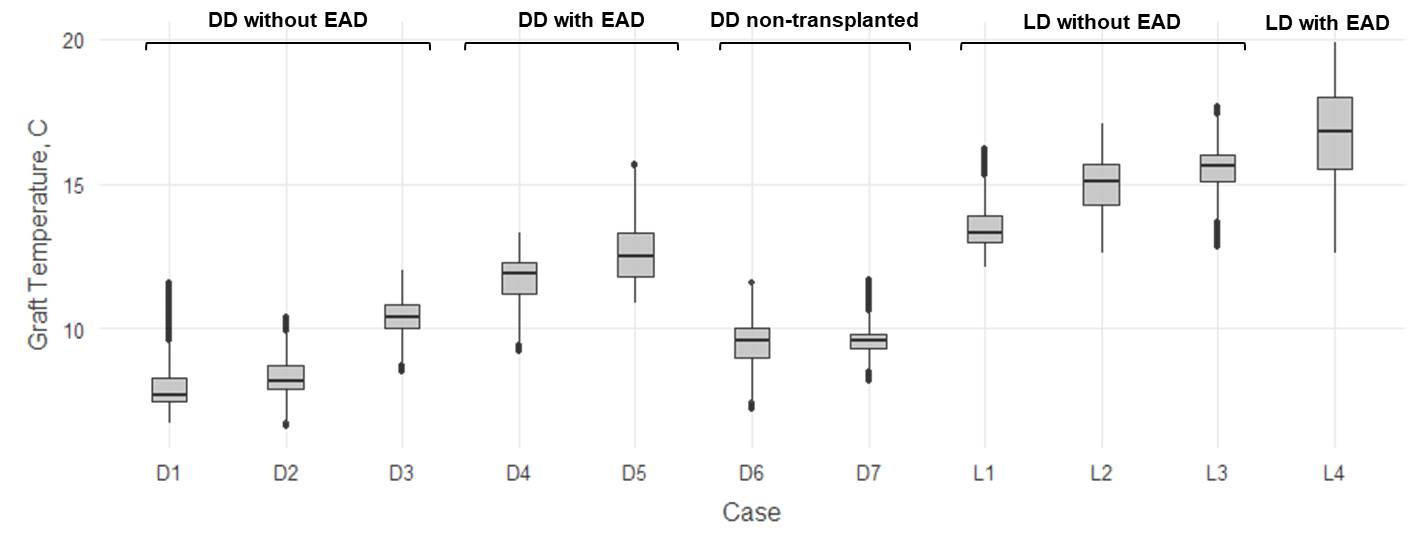
At the end of CIT the Temp of DD grafts with normal initial function (D1, D2 and D3) were significantly lower than in grafts with EAD (D3 and D4): 8,5 [7,8 – 10,1](6,6 – 12,0) vs. 12,1 [11,5 – 12,7](9,2 – 15,7), p = 0.005.
In addition to the level of Glyc, there were no other significant differences in microdialysis parameters between DD and LD grafts.
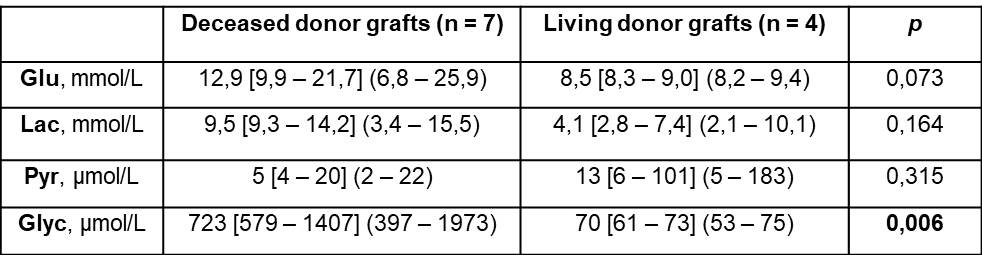
This was probably due to a strong correlation between Glyc level and CIT: Spearman R = 0,96; p <0,001.
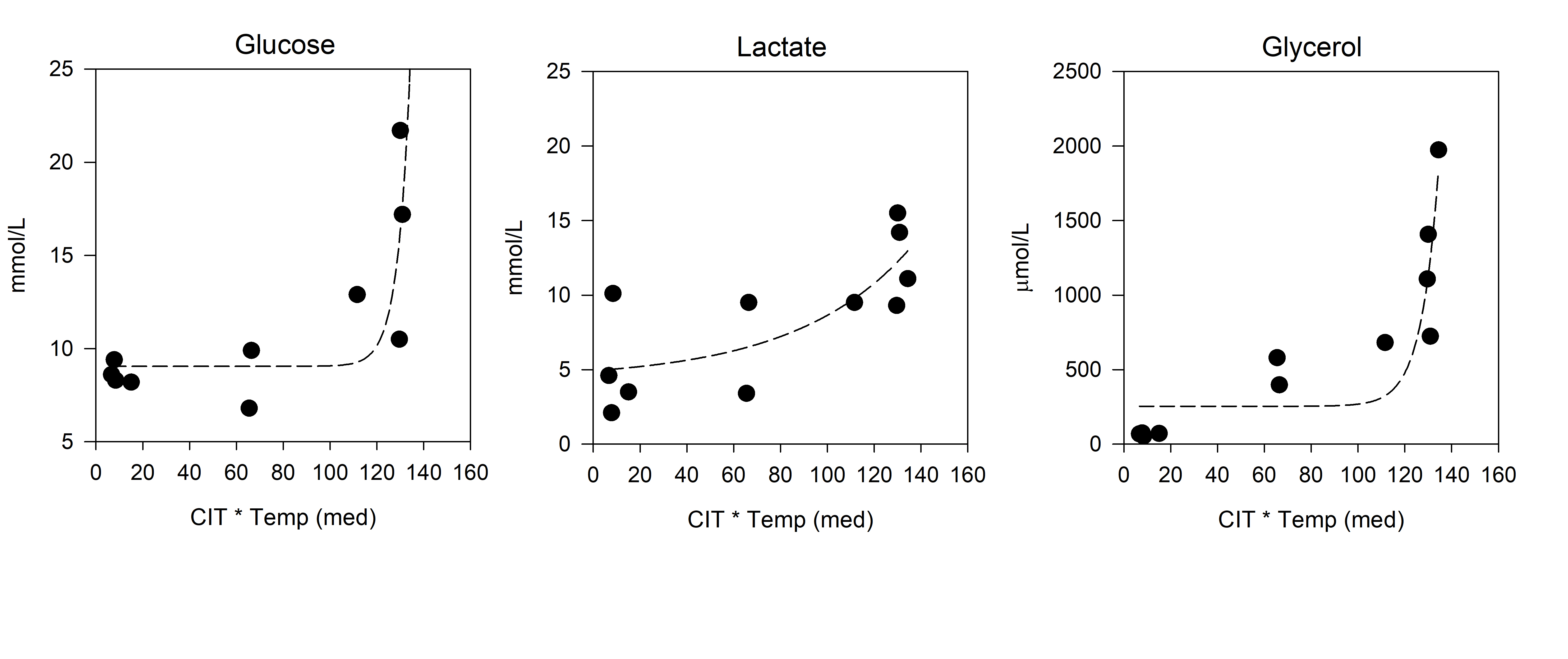
Based on the suggesting that not only CIT but also T(med) affects the graft metabolic state immediately before transplantation, a new variable was introduced: [CIT * T(med)] (hours * ⁰C).
Apparently, the relationship of this parameter with interstitial levels of Glu, Lac, and Glyc was nonlinear. The best results of dynamic fitting in all cases were achieved using the equation: f = y0+a*exp(b*x). The R2 values for Glu, Lac and Glyc were 0,80, 0,60 and 0,81, respectively.
Conclusion: Our results confirm the strong influence of Temp on the state of metabolism in the graft and its initial function. The development of devices for continuous assessment of metabolic state and Temp control during cold storage is promising.
Russian Science Foundation (grant # 19-75-10040).
There are no comments yet...

