

Cytomegalovirus infection after kidney transplantation with pre-emptive strategy: A single-center retrospective cohort study
Chumpol Santisiripat1, Korntip Phonphok1.
1Nephrology Unit, Department of Internal Medicine, Rajavithi Hospital, Bangkok, Thailand
Background: Despite the fact that pre-strategy and universal prophylaxis are of paramount significance in decreasing the risk of post-kidney transplantation (KT) Cytomegalovirus (CMV) infection, using those standard approaches are not always feasible in countries with limited resources including Thailand. Here in order to alleviate the consequential infection, we have implemented our in-house monitoring protocol for detection of CMV infection after KT. The urge for early CMV detection along with pre-emptive strategy might play a major role in predicting transplant outcome since knowledge on incidence of CMV infection following KT were highly anticipated in our transplant center.
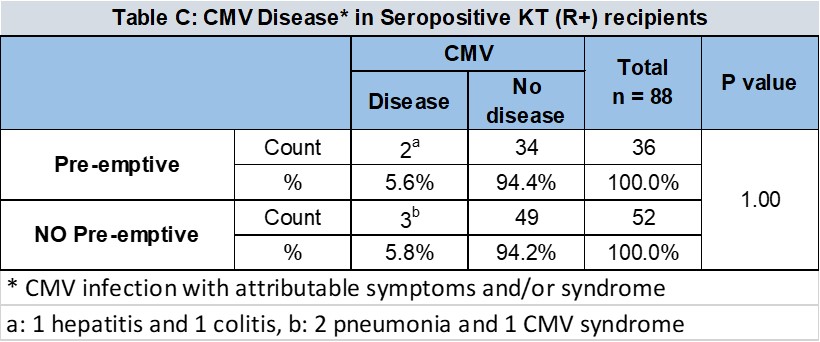
Materials and Methods: Retrospective cohort analysis of adult kidney transplant recipients who underwent KT between January 2015 and June 2019, was performed. All patients who had CMV-seropositivity prior to KT were eligible in this study. Pre-emptive CMV therapy was defined as the monitoring of CMV viral load at every two week for 3 months, then every three months until one-year post KT. The study outcome was CMV infection and symptomatic CMV disease within 1 year following KT. CMV infection was defined as any of asymptomatic significant viremia, CMV viral load >5,000 copies/ml, measured by polymerase chain reaction. CMV disease was defined as the occurrence of CMV infection with attributable symptoms and/or syndrome. This study was approved by Rajavithi’s Ethical committee. The statistical analysis was performed with SPSS software version 24.
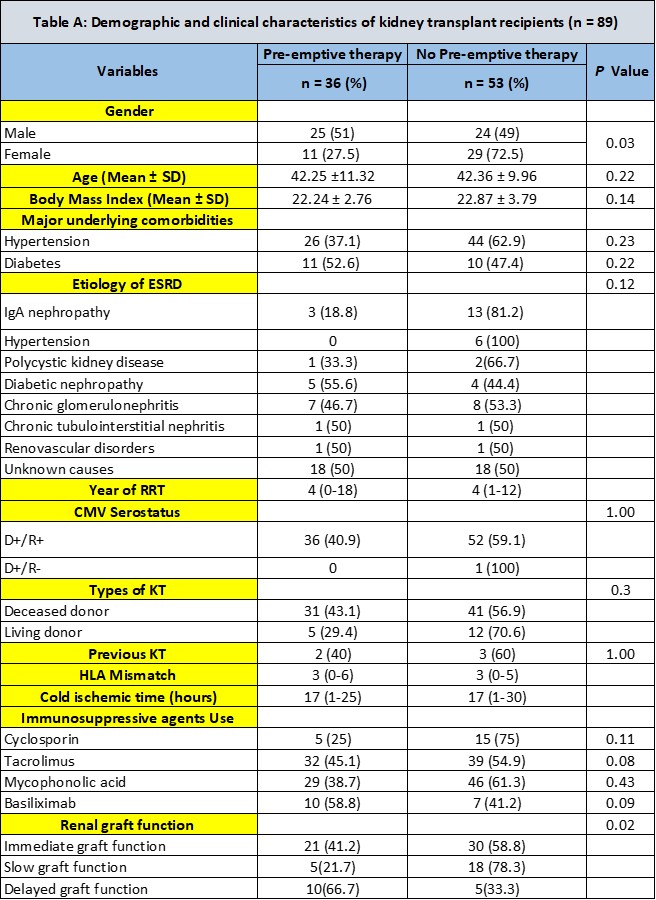
Results: The data revealed 88 kidney transplant recipients, of these, 36 (40.9%) received pre-emptive CMV therapy. CMV infection was more evident in patients receiving pre-emptive therapy [11 (30.6%) vs 3 (5.8%), P <0.01], whereas symptomatic CMV disease was not different between groups (5.6% vs 5.8%, P = 1.00), [2 (1 hepatitis and 1 colitis) In pre-emptive vs 3 (2 pneumonia and 1 syndrome)]. Under pre-emptive strategy, patients with CMV infection were more likely to be older [(49.6 vs 41 Years old), P = 0.04], and have longer time on dialysis prior to KT [(6.2 vs 4.2 years), P = 0.01], compared to those not receiving.

Conclusion: Our experience showed that pre-emptive CMV monitoring was helpful in the detection of asymptomatic significant viremia, but did not lower the incidence of symptomatic CMV disease. These results confirmed the evidences of pre-emptive therapy, even our in-house monitoring protocol, could show the benefit from early detection of subclinical CMV infection, necessitating the prevention of cost- and life-saving of CMV disease burden. Future studies on CMV–related effects following prompt diagnosis such as graft rejection and survival outcome would substantiate the need for CMV prevention among intermediate to high risk KT population.
[1] Camille NK, Deepali K, Angela MC, Shirish H, Sunwan C, Lara DI, et al. The Third internal consensus guideline on the Management of Cytomegalovirus in Solid-organ transplantation. Transplantation. 2018; 102: 900-931.
[2] Pretagostini R, Poli L, Lai Q, Russo G, Nudo F, Garofalo M, et al. Pre-Emptive therapy for the treatment of Cytomegalovirus after kidney transplantation. Transplant Proc. 2017; 49: 638-41.
There are no comments yet...

