
CHAIR Score: A novel risk stratification in transplant renal artery stenosis
Xiangyong Tian1, Wenjing Duan1, Tianzhong Yan1, Xiaoqiang Wu1, Guanghui Cao1.
1Kidney Transplantation, Henan Province People's Hospital, Zhengzhou, People's Republic of China
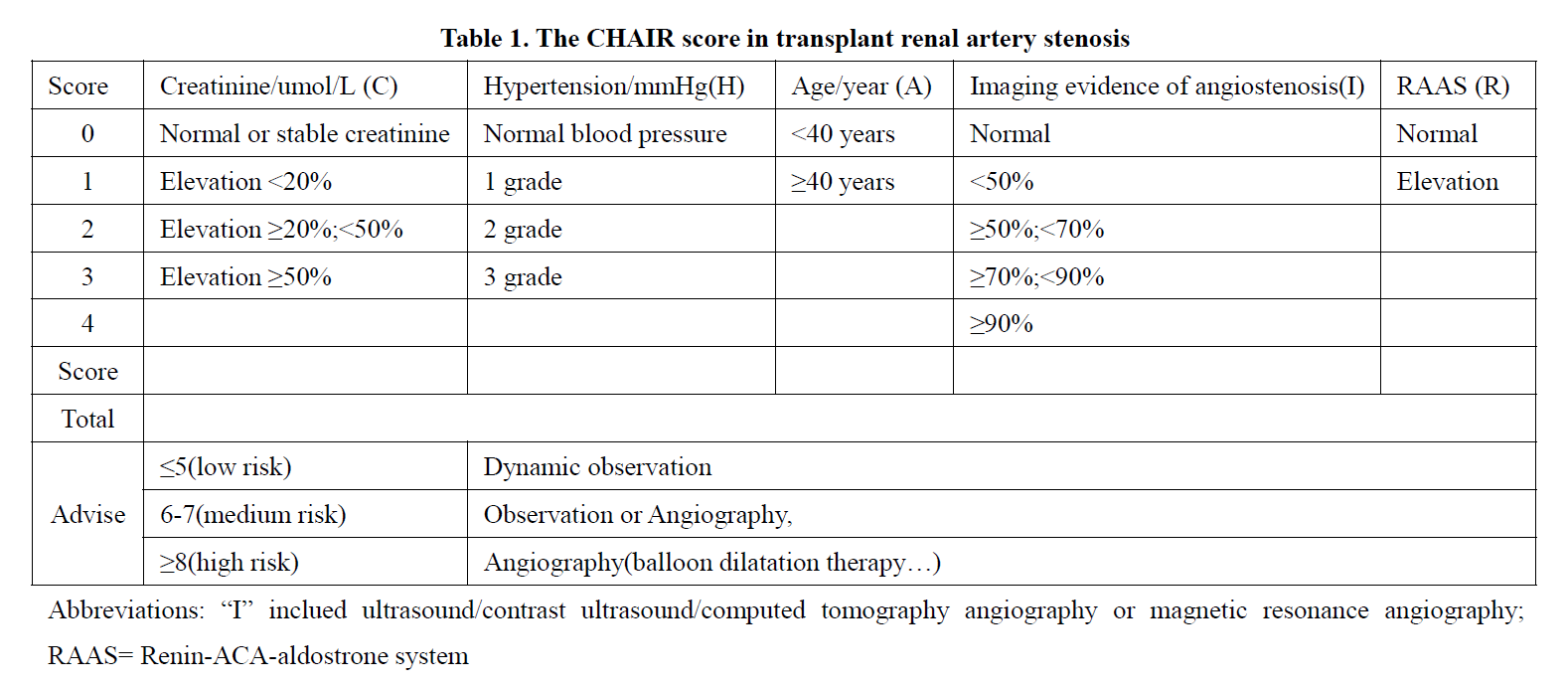
Purpose: The aim of the study is to evaluate the clinical application of CHAIR score based on creatinine (C), hypertension (H), age (A), imaging evidence of angiostenosis (I), and Renin-ACA-aldostrone system (RAAS, R) in diagnosing the severity of transplant renal artery stenosis (TRAS) for selection of patients potentially requiring endovascular intervention and predicting the timing of intervention.
Methods: A retrospective, institutional review board-approved study of TRAS patients at a single institution was conducted. From April 2016 to June 2019, 353 patients with renal transplantation were reviewed and 25 patients of them with TRAS were found and confifirmed by imaging evidence. The score of each of the 25 patients is calculated according to the criteria in Table 1 based on risk stratifification. A total CHAIR score of 8 or greater is considered high risk and a score of 5 or less is considered low risk. The Mid-range scores (6 and 7) is considered medium risk. All data were obtained through the electronic health record.
Results: According to the CHAIR score among them, three cases in the low risk were observed dynamically. Five cases was in the medium risk and two of them received arteriography of transplanted kidney followed by only one case treated with balloon dilation, and the other three cases were observed dynamically. There were 17 cases in the high risk, who were all treated with angiography, and to whom balloon dilatation therapy was given immediately after TRAS was confifirmed. The creatinine of 19 patients was (292.9 ± 165.6) umol / L before intervention, and decreased to (190.3 ± 130.5) umol / L after intervention. The di!erence was statistically signifificant (P < 0.05). The peak systolic blood flflow of the stenosis site was (328.2 ± 194.8) cm / S before intervention and (180.2 ± 129.7) cm / s after intervention. The di!erence was also statistically signifificant (P < 0.05). The CHAIR score were related to the severe extent of TRAS.
Conclusions: The CHAIR score has the function of evaluating the severity of TRAS and prompting the timing of intervention to some extent, which may allow for a more appropriate and individualized treatment for TRAS patients. Patients with scores ≥ 8 often need to take timely intervention to benefifit from it.
Science and Technology Development Plan of Henan Province (202102310438). “23456 Talent project ” of Henan Provincial People’s Hospital.
There are no comments yet...

