
How calcineurin inhibitor dosage and blood trough levels affect kidney allograft survival?
Didem Turgut1, Zeynep Kendi Celebi1, B. Handan Ozdemir2, Turan Colak1, Ebru H. Ayvazoglu Soy3, Mehmet A. Haberal3.
1Nephrology, Baskent University, Ankara, Turkey; 2Pathology, Baskent University, Ankara, Turkey; 3Transplantation, Baskent University, Ankara, Turkey
Introduction: Calcineurin inhibitors (CNI) (cyclosporine and tacrolimus) led to major advances in the field of kidney transplantation. However in the long-term period CNI can cause chronic nephrotoxicity. And also with the effect of over-immunsuppression they may be related to BK virus nephropathy (BKVN). But it is not clear that if drug dose or blood trough levels are related to immunosuppression level or toxicity. In this study, we aimed to understand if CNI drug dose and blood levels were related to chronic CNI nephrotoxicity or BKVN.
Materials and Methods: We analyzed 1598 kidney allograft biopsy reports retrospectively who have been performed between 1998 and 2018 in Baskent University Ankara Hospital. 270 allograft biopsies reported as only BKVN and only chronic CNI toxicity were included in the study. Patients were compared due to their immunsuppressive regimes as cyclosporine+mycophenolate+steroid and tacrolimus+mycophenolate+steroid. Additionally, tacrolimus metabolism rate is calculated (Concentration/Dose (C/D) ratio-ng/mL*1/mg). Patients with C/D >1.55 was slow metabolizer, C/D<1.05 was fast metabolizer and C/D between 1.06-1.55 were intermediate metabolizer.
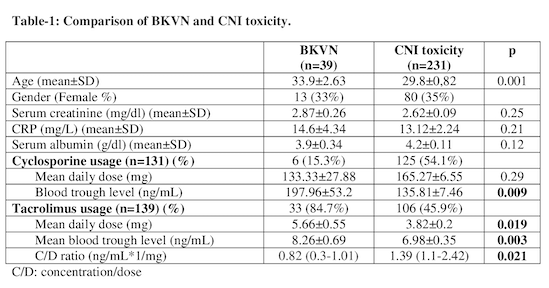
Results: 39 patients with BKVN and 231 patients with CNI toxicity were analyzed. Mean age was higher in the BKVN group (p=0.001). For cyclosporine, mean daily drug dose were similar (133.33±27.88; 165.27±6.55; p=0.29) while drug blood levels were higher in BKVN group (197.96±53.2; 135.81±7.46; p=0.009). For tacrolimus, mean daily dose (5.66±0.55; 3.82±0.20; p=0.001) and blood through levels (8.26±0.69; 6.98±0.35; p=0.003) were higher in BKVN group. In BKVN group tacrolimus C/D ratio was lower (0.82ng/mL) than CNI group (1.39 ng/mL) for tacrolimus (p=0.21). In BKVN group all patients were fast metabolizer for tacrolimus (Table-1).
Conclusion: During maintaining an optimal allograft function, high drug concentrations of CNI or high metabolism rate (C/D>1.55 ng/mL*1/mg) for tacrolimus may be a risk factor for BKVN and related to over-immunsupression. But for CNI toxicity drug blood concentrations are not the only affecting factor. For this group who are on tacrolimus and slow/intermediate-metabolizer are more under risk. This results may be related to high inter- and intraindividual pharmacokinetic variability of CNI.
There are no comments yet...

