
Clinical benefits of coronary CT angiography in preventing cardiovascular complications among renal transplant recipients
Si Youn Kim1, Sangmi Lee2, Sojung Yoon1, Hyung Woo Kim2, Kyu Ha Huh3,4, Beom Seok Kim2,4.
1College of Medicine, Yonsei University, Seoul, Korea; 2Division of Nephrology, Department of Internal Medicine, Severance Hospital, Yonsei University Health system, Seoul, Korea; 3Department of Surgery, Yonsei University College of Medicine, Seoul, Korea; 4The Research Institute for Transplantation, Yonsei University College of Medicine, Seoul, Korea
Introduction: Cardiovascular disease is the leading cause of death in KT recipients. The aim of this study is to investigate whether performing coronary CT angiography in KT recipients is clinically beneficial in preventing cardiovascular complications in long term.
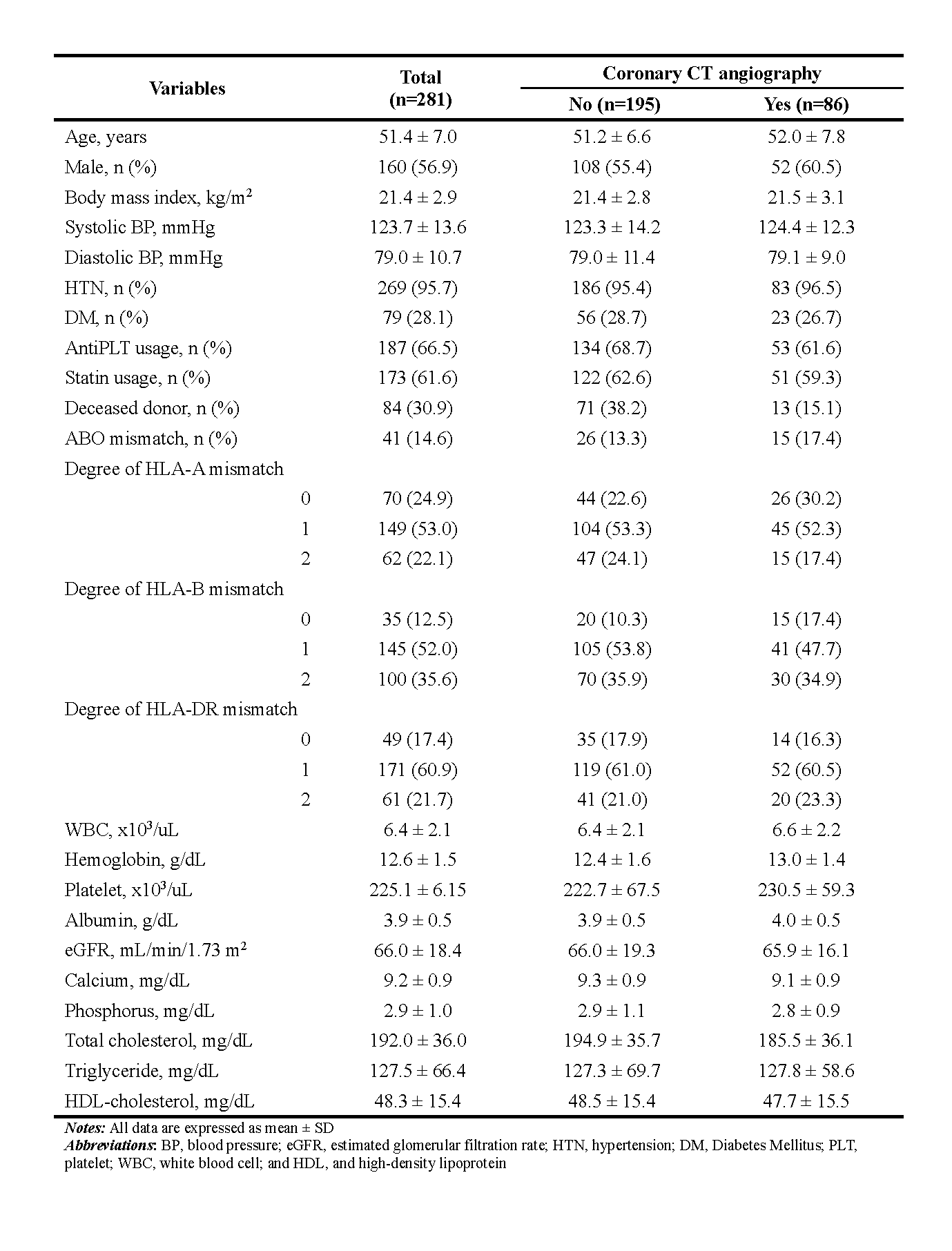
Methods: Respective analysis was performed on 281 patients who underwent renal transplant between March 2011 and May 2014 at Severance Hospital of Yonsei University College of Medicine. Only patients with no history of coronary artery disease and with no signs or symptoms suggestive of cardiovascular disease during the past month were enrolled in the study. Study population was categorized into 2 groups; the intervention group that underwent coronary CT (n=86) and the control group that didn’t go through coronary CT (n=195). The severity of CAD according to coronary CT was also divided into mild CAD, 1 vessel obstructive, 2 vessels obstructive (or in the proximal left anterior descending), and 3 vessels obstructive (or left main).
Results:
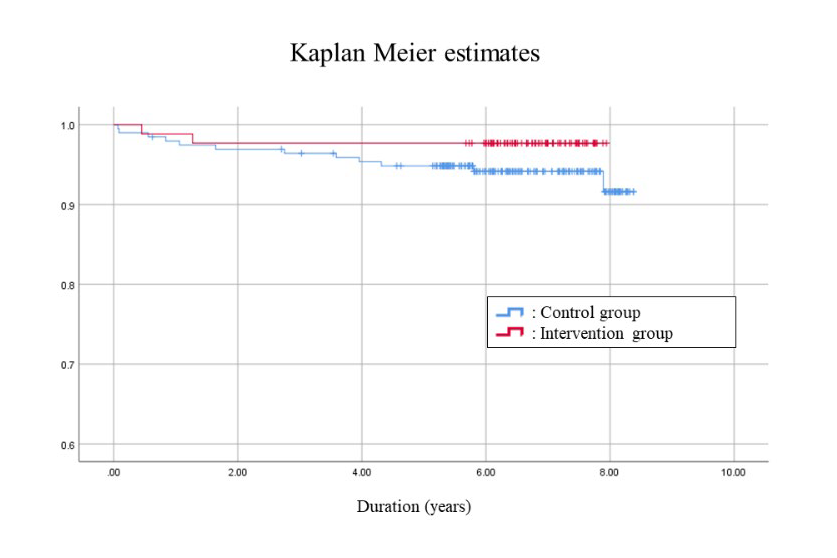
During a mean follow up duration of 6.5 years, the incidence rate of MACE in total patients was 7.68 (95% CI: 4.55 - 13.0) events per 1000 person-year. And the incidence rate of MACE was much lower in the intervention group who had proper management after coronary CT surveillance: 3.46 (95% CI: 0.87 – 13.8) and 9.63 (95% CI: 5.47 - 17.0) events per 1000 person-year in intervention and control group, respectively.
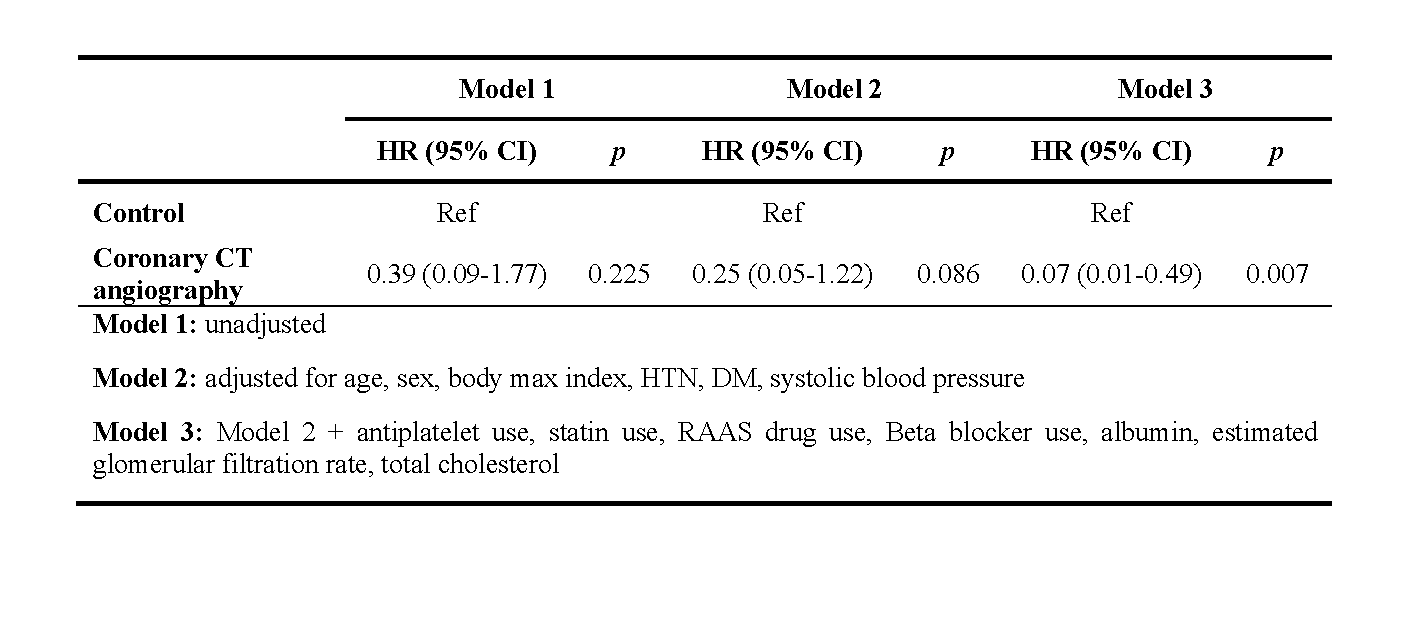
Through multivariate Cox proportional hazard model adjusted with confounding factors, surveillance through coronary CT was determined as an independent factor that reduces the risk of cardiovascular complications in renal recipients (HR=0.07 [95% CI: 0.01 - 0.49], P=0.007).
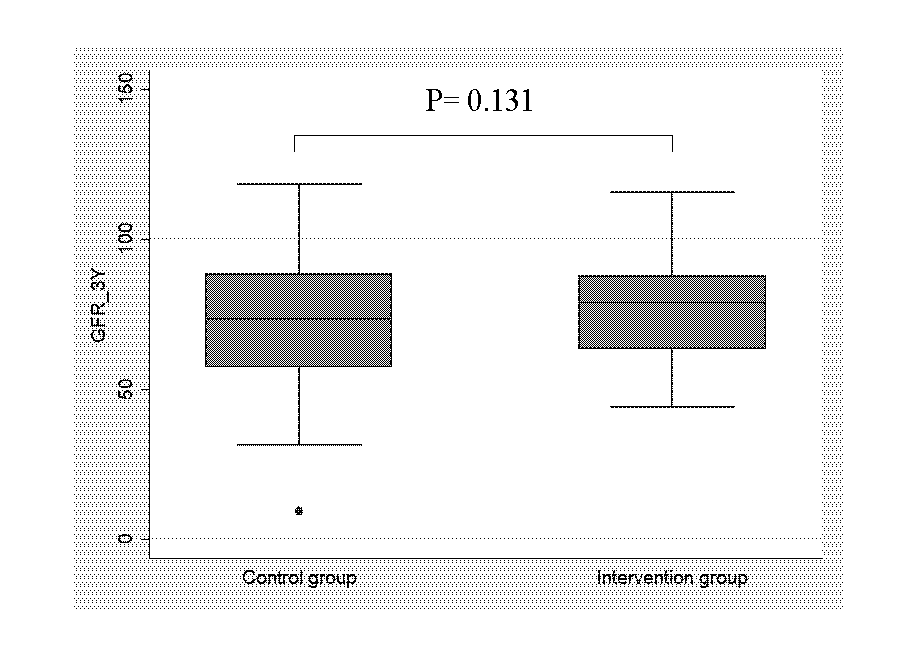
The mean 3-year eGFR were 73.5 ± 19.7 and 77.2 ± 15.9 mL/min/ 1.73 m2 in intervention and control group, respectively, and there was no significant difference between two groups (P=0.131).
Conclusions: High detection rate of CAD through coronary CT and with proper management combined, it leads to much lower incidence rate of MACE compared with the control group in long term. And no significant difference in long term graft functions were found in intervention group and control group.
Student Research Fund of Yonsei University College of Medicine in 2018.
[1] Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341(23):1725-30.
[2] Laupacis A, Keown P, Pus N, Krueger H, Ferguson B, Wong C, et al. A study of the quality of life and cost-utility of renal transplantation. Kidney Int. 1996;50(1):235-42.
[3] Port FK, Wolfe RA, Mauger EA, Berling DP, Jiang K. Comparison of survival probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA. 1993;270(11):1339-43.
[4] Schnuelle P, Lorenz D, Trede M, Van Der Woude FJ. Impact of renal cadaveric transplantation on survival in end-stage renal failure: evidence for reduced mortality risk compared with hemodialysis during long-term follow-up. J Am Soc Nephrol. 1998;9(11):2135-41.
[5] Arend SM, Mallat MJ, Westendorp RJ, van der Woude FJ, van Es LA. Patient survival after renal transplantation; more than 25 years follow-up. Nephrol Dial Transplant. 1997;12(8):1672-9.
[6] Lindholm A, Albrechtsen D, Frodin L, Tufveson G, Persson NH, Lundgren G. Ischemic heart disease--major cause of death and graft loss after renal transplantation in Scandinavia. Transplantation. 1995;60(5):451-7.
[7] Vanrenterghem YF, Claes K, Montagnino G, Fieuws S, Maes B, Villa M, et al. Risk factors for cardiovascular events after successful renal transplantation. Transplantation. 2008;85(2):209-16.
[8] Matas AJ, Gillingham KJ, Humar A, Kandaswamy R, Sutherland DE, Payne WD, et al. 2202 kidney transplant recipients with 10 years of graft function: what happens next? Am J Transplant. 2008;8(11):2410-9.
[9] Kasiske BL, Guijarro C, Massy ZA, Wiederkehr MR, Ma JZ. Cardiovascular disease after renal transplantation. J Am Soc Nephrol. 1996;7(1):158-65.
There are no comments yet...