
Predicting kidney function after high KDPI kidney transplantation: A comparison of expected vs. observed glomerular filtration rate in a large cohort of KDPI >85 kidney transplant recipients
Trisha Blake-Popham1, Heather Kutzler1, Zeynep Ebcioglu1, Glyn Morgan1,2, Caroline L. Rochon1,2, Patricia A. Sheiner1,2, Joseph U. Singh1, Joseph Tremaglio1, Xiaoyi Ye1, Oscar Serrano1,2.
1Transplant Program, Hartford Hospital, Hartford, CT, United States; 2Surgery, University of Connecticut School of Medicine, Farmington, CT, United States
Purpose: Renal function after transplantation is dependent on a combination of viable donor nephron mass and the adaptation of recipient glomerular filtration. Although previous studies have assessed post-transplant kidney function from living and standard criteria deceased donor kidney transplant recipients, no study has sought to calculate kidney function following high KDPI (KDPI>85) kidney transplantation.
Methods: From December 2014 to July 2019, 58 kidney transplants with KDPI>85 were performed at Hartford Hospital. Using the modified Glomerular Filtration Rate Cockcroft and Gault equation (CG-GFR) expected serum creatinine (ExpSCr) at one year was calculated and compared to observed serum creatinine (ObsSCr). Bland-Altman analysis was performed to assess concordance between ExpSCr and ObsSCr. Bias (mean difference between ExpSCr and ObsSCr) and limits of agreement with their 95% confidence intervals were determined.
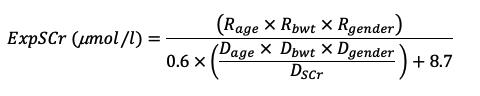
Results: Among 58 high KDPI kidney transplants, the average KDPI was 91±4%. The donor age was 61±6 years, 57% were male with an average BMI of 31.5±8.0 kg/m2. Of the donor cohort, 82% had a history of hypertension, 40% diabetes, 59% died of cardiovascular causes, and 30% donated after cardiac death. Of the recipient cohort, the average age was 63±8 years, 69% were male with a BMI of 29.4±5.1 kg/m2. More than half of the recipients (69%) were male; 45% self-identified as Caucasian, 31% African American, 17% Hispanic and 7% Other; and 50% and 90% had a pre-transplant diagnosis of diabetes and hypertension, respectively. Delayed graft function was observed in 53% of recipients. The 1-year death-censored graft and patient was survival was 95.7% and 91.5% (n=47), respectively. The 6-month and 1-year creatinine for the cohort were 1.86±1.18 (n=49) and 1.68±0.52 mg/dL (n=41), respectively. According to the CG-GFR, the ExpSCr at the first post-transplant year was 1.33±0.47 mg/dL. The average lowest ObsSCr was 1.32±0.47 mg/dL. The bias of expected and ObsSCr and ExpSCr of this cohort of high KDPI kidney transplant recipients was 0.01 mg/dL.

Conclusion: Current models for predicting kidney function after living and standard criteria deceased donors accurately predict post-transplant kidney function in high KDPI kidney transplantation. Further research is necessary to identify mitigating risk factors to achieve the optimal donor-recipient match and best possible post-transplant kidney function for high KDPI kidneys.
[1] Al-Sehli R, et al. What Should the Serum Creatinine Be After Transplantation? An Approach to Integrate Donor and Recipient Information to Assess Posttransplant Kidney Function. Transplantation. 2015 Sep;99(9):1960-7.
There are no comments yet...