
Correlation of trough level compliance and protection of renal function after liver transplantation – A post-hoc analysis from the Hephaistos study
Björn Nashan1, Peter Schemmer1, Hans J. Schlitt1, Andreas Pascher1, Christian G. Klein1, Ulf P. Neumann1, Irena Kroeger2, Peter Wimmer2, Felix Braun1.
1Hephaistos, Study, Group, Germany; 2Novartis Pharma, GmbH, Nürnberg, Germany
Introduction: The majority of immunosuppressive agents are administered according to trough levels (C0-levels). Avoiding both over- and underimmunosuppression is crucial to achieve an optimal balance between efficacy and safety. Although many studies have been performed to optimize immunosuppression, it has been revealed that pre-defined C0-levels are often not kept for distinct reasons. The aim of the Hephaistos study(1) was to investigate the impact of a reduced calcineurin inhibitor (CNI) regimen on renal function as well as CNI-induced nephrotoxicity following liver transplantation (LTx).
Materials and Methods: The primary endpoint of this 12 months (M) open-label, prospective, randomized de novo liver transplant study was to show that at M12 immunosuppressive therapy based on everolimus (EVR: 3-5ng/ml) combined with reduced tacrolimus (rTAC: <5ng/ml) yields superior renal functionality compared to TAC alone (TAC-C: 6-10ng/ml). In this study, a numerical yet not significant improvement was shown in the full analysis set. Nevertheless, TAC C0-levels of 31-42% of patients in the EVR+rTAC arms were detected to be above the pre-defined range at various time points. Therefore, a posthoc analysis of a compliance set was conducted in which patients were only included if their C0-levels were within the TAC target range for a minimum of three different time points during the study.
Results and Discussion: Out of 333 randomized patients, 59 of 164 in the TAC-C arm and 74 of 169 patients in the EVR+rTAC made up the compliance set. At M12 a significantly higher mean eGFR (MDRD4) was obtained with EVR+rTAC (adjusted mean difference of 8.03 ml/min/1.73m2; p=0.0333). Contrarily, a difference of only 1.20 ml/min (p=0.7154) was observed in the non-compliance set (95 EVR+rTAC, 105 TAC-C). Regarding efficacy and safety, no difference was seen irrespective of compliance or treatment regimen.
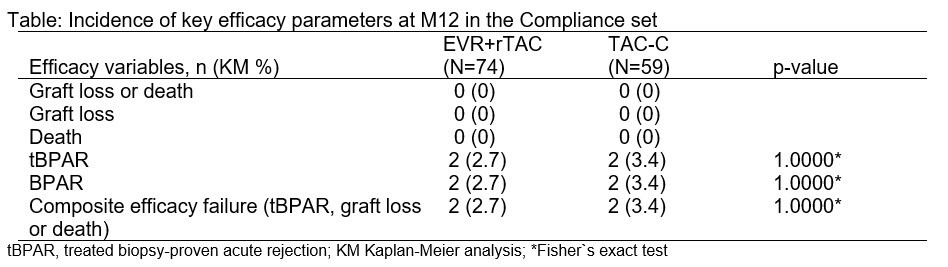
Conclusion: This compliance set analysis clearly revealed that when TAC C0-levels did not exceed the pre-defined range, renal function was significantly improved at M12 in the EVR+rTAC arm compared to the TAC-C group, with efficacy and safety being unaffected. Hence, EVR plus rTAC is an effective and well-tolerated regimen, allowing CNI minimization and yielding renal benefit after LTx.
[1] Nashan et al. Trials. 2015; 16:118

