
BK virus allograft nephropaty in renal transplant recipients
Fernando Giron-Luque 1,2, Andrea Garcia-Lopez 1, Nasly Patino-Jaramillo1, Javier Amaya-Nieto1.
1Research , Colombiana de Trasplantes, Bogota, Colombia; 2Transplant Surgery, Colombiana de Trasplantes, Bogota DC, Colombia
Introduction: The BKV nephropathy (BKVN) is an important cause of chronic allograft dysfunction in renal transplant recipients. Thus, there is a clear need to investigate and prevent the BKVN in kidney transplant patients. The aim of this study was to assess clinical outcomes of as a result of (BKVN).
Methods: A total of 1528 kidney transplants were performed from January 2008 and December 2019. We retrospectively reviewed 28 kidney allograft biopsies from patients with Interstitial Tubular Nephritis. All patients had evidence of polyomavirus nephropathy (BKVN) with intra-nuclear viral inclusions in the tubular epithelial cells stained with hematoxylin-eosin. Data regarding transplant recipient and donor demographics, glomerular filtration rate (GFR) and immunosuppressive medication at the time of the biopsy, BKVN therapeutic strategy, and graft function evolution were collected. Date of diagnosis of BKVN was defined as the date of the first biopsy with positive immunohistochemistry for BKV. The statistical analysis was event-driven, being the event of interest initiation of dialysis. Overall probabilities of not initiating dialysis were obtained and plotted by use of the Kaplan-Meier method. Analysis of patient clinical characteristics, serum creatinine and clinical outcomes were assessed.
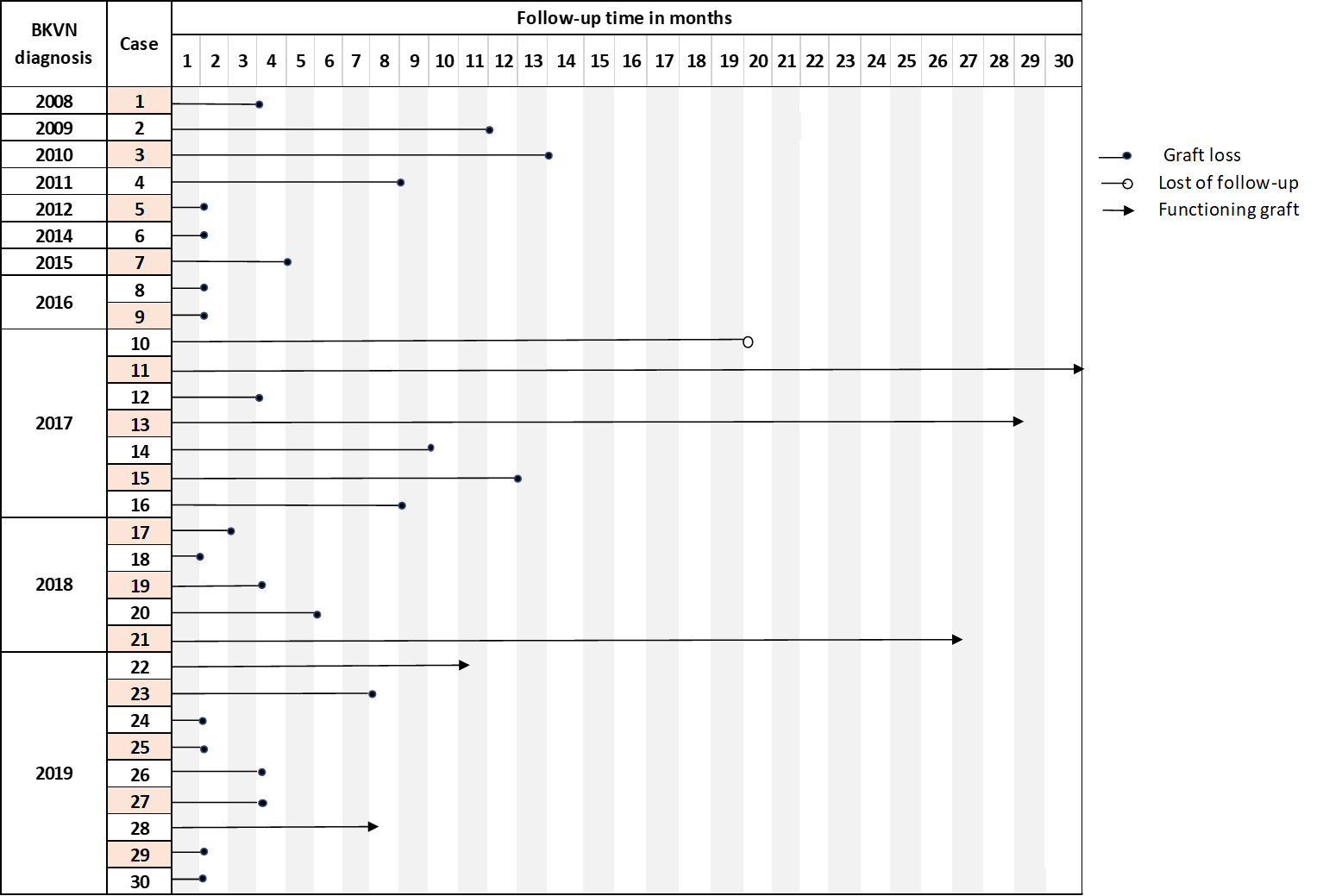
Results: BKVN was histologically diagnosed in 30 recipients.
Mean of follow-up time was 7 months (range 1-30 months).
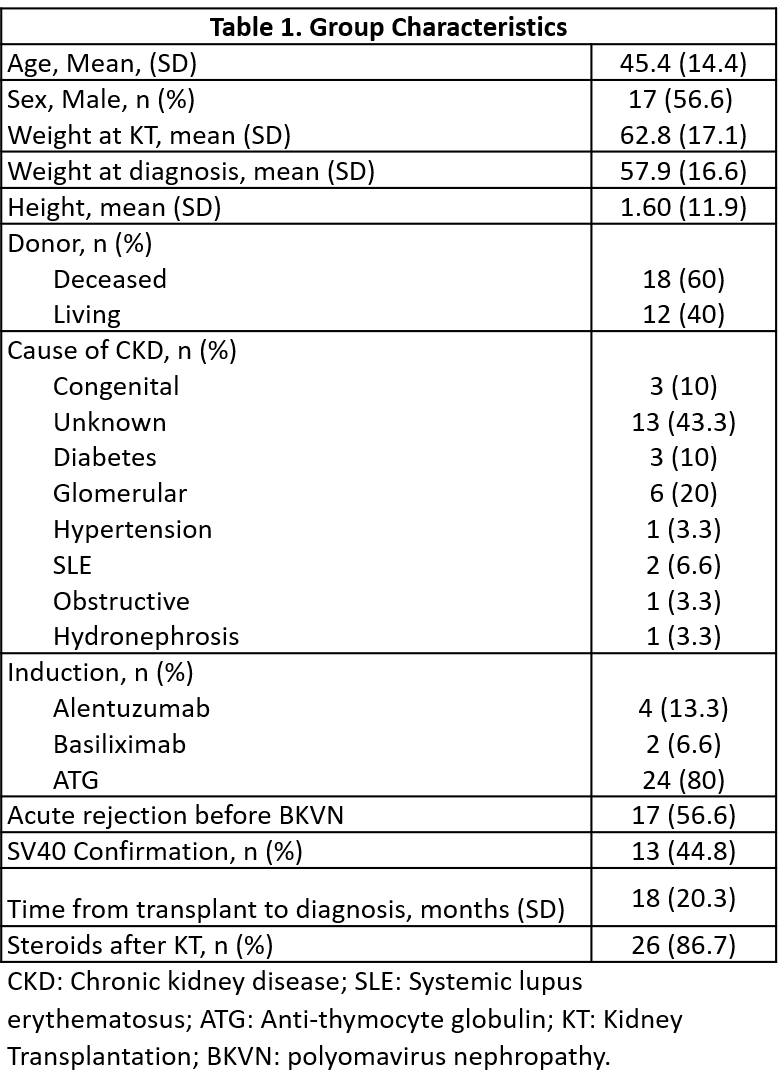
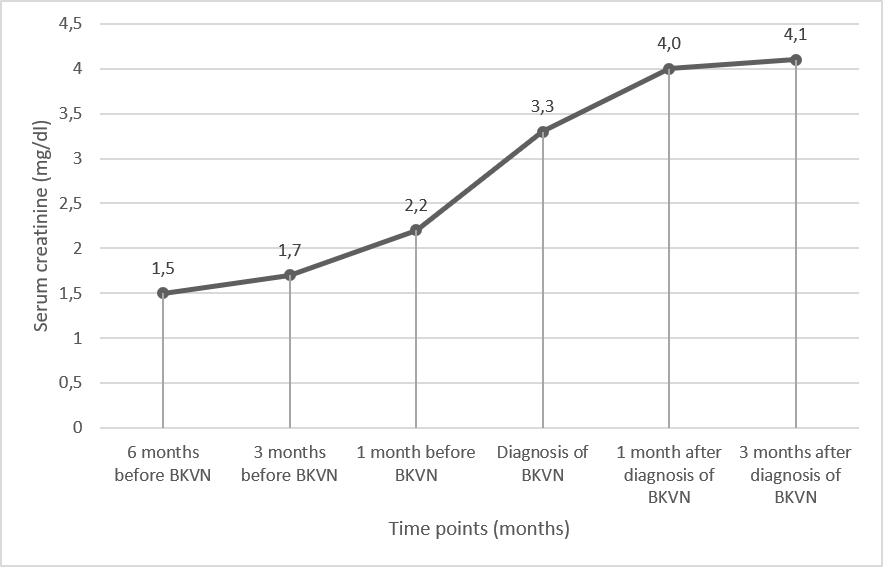
The incidence rate was 3.7% during the 10-year study period. Mean of time to diagnosis was 18.3 ± 20.7 months after transplant. Mean age was 45.4 ± 14.4 years and 18 had a deceased donor. Diabetes affected 3 patients, acute rejection (AR) was diagnosed in 17 patients before of BKVN diagnosis. Among, all of them were medicated with methylprednisolone pulse therapy. All patients were medicated with calcineurin inhibitors (CNI) (93.3% tacrolimus), and all recipients also received an antimetabolite. Mean of serum creatinine was 1.5mg/dl at 6 months before BKVN, compared to 3.9mg/dl at 3 months after BKVN.
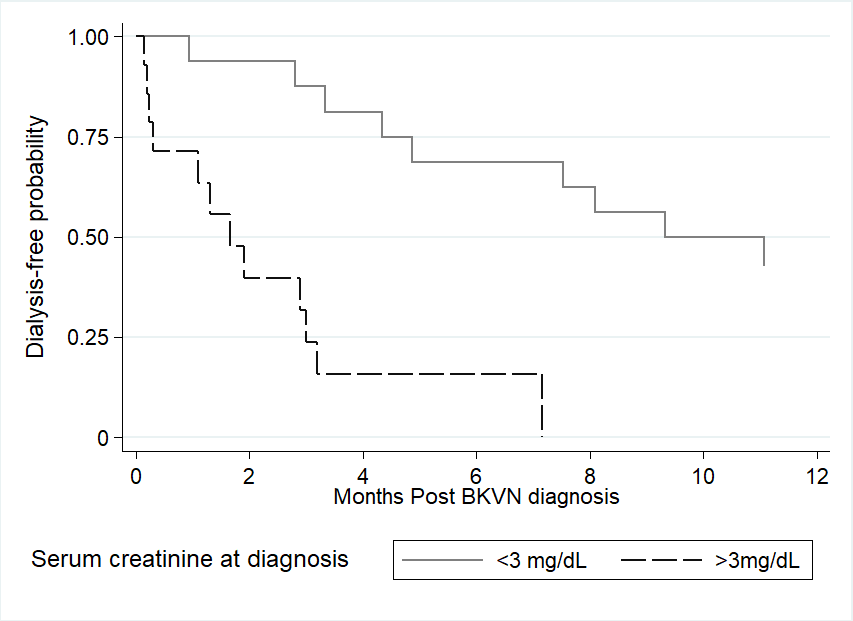
Graft loss (GL) occurred in 24 patients (80%). Serum creatinine >3mg/dl was associated with an increased risk of initiation of dialysis (HR: 7.1; CI 95% 2.4- 21.4; p 0.00).
Conclusion: GL occurred in 80% of patients with BKVN, serum creatinine levels at the time of diagnosis was an important risk factor. Early diagnosis of BKVN is essential to prevent GL.
[1] Costa JS, Ferreira E, Leal R, Bota N, Romãozinho C, Sousa V, et al. Polyomavirus Nephropathy: Ten-Year Experience. Transplant Proc [Internet]. 2017;49(4):803–8. Disponible en: http://dx.doi.org/10.1016/j.transproceed.2017.01.072
[2] Chan BD, Wong G, Jiang Q, Lee MM-L, Wong W-Y, Chen F, et al. Longitudinal study of BKV outcomes, risk factors, and kinetics in renal transplantation patients. Microb Pathog [Internet]. 2020;104036. Disponible en: https://doi.org/10.1016/j.micpath.2020.104036
[3] Leeaphorn N, Thongprayoon C, Chon WJ, Cummings LS, Mao MA, Cheungpasitporn W. Outcomes of kidney retransplantation after graft loss as a result of BK virus nephropathy in the era of newer immunosuppressant agents. Am J Transplant. 2019;0–3.
There are no comments yet...

