
Herpes simplex virus type 1 encephalitis in kidney transplant patient: A case report
Jessica Pinto-Ramirez1, Nasly Patino-Jaramillo2, Andrea Garcia-Lopez 2, Fernando Giron-Luque 2,3.
1Nephrology, Colombiana de Trasplantes, Bogota DC, Colombia; 2Research, Colombiana de Trasplantes, Bogota DC, Colombia; 3Transplant Surgery, Colombiana de Trasplantes, Bogota DC, Colombia
Introduction: Herpes simplex type 1 infection (HSV type 1) has an incidence of 3% in transplant patients who have used antiviral prophylaxis compared to 9.8% without prophylaxis in the first year after the transplantation (1). Herpes virus infection usually causes mucocutaneous lesions and it could result in systemic or central nervous infection in a reduced proportion (1–3). HSV type 1 encephalitis is an uncommon infection in immunocompromised patients (4). Cerebrospinal Fluid (CSF) Polymerase Chain Reaction (PCR) is the gold standard for diagnosing HSV type 1 encephalitis with a sensitivity of 100% and specificity of 99.9% (5). According to recent publications, acyclovir has been chosen as its medical treatment (1).
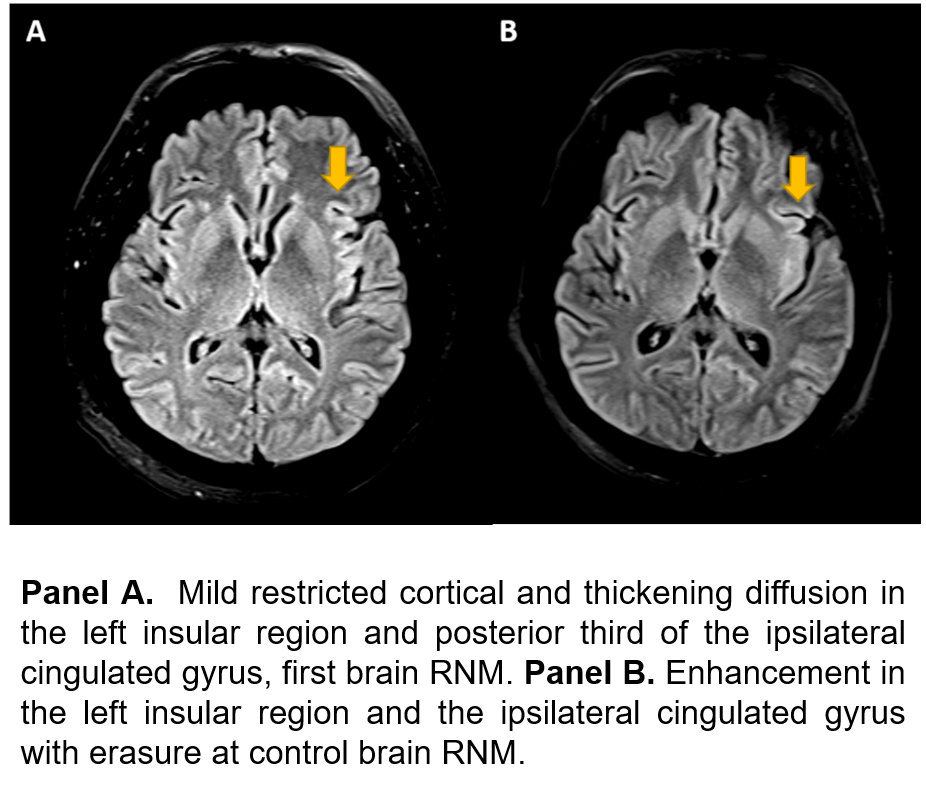
Materials and Methods: 56 years old male, stockbreeder, with a medical history of chronic kidney disease of unknown etiology, underwent to kidney deceased donor transplant in July 2006. His donor was not screened for HSV type 1 according to national organ procurement guidelines in 2006 (6). Herpesviridae serology was positive for HSV type 1 in the patient before the transplant. Thymoglobulin was indicated as induction therapy. Tacrolimus (5 mg/day) and mycophenolate mofetil (1440 mg/day) were used as immunosuppression scheme. In 2014, the patient presented acute kidney rejection treated with corticoids and thymoglobulin. In 2018, the patient was admitted due to tachycardia, malaise, moderate dehydration, and liquid diarrhea. At 24 hours after admission, the patient had convulsive syndrome, requiring orotracheal intubation and anticonvulsive treatment. Serum creatinine was at 3.73 mg/dL, CSF PCR was positive for HSV type 1 and brain magnetic resonance (RNM) was obtained (Figure 1). Following the diagnosis of HSV type 1 encephalitis, the patient was treated with acyclovir 6 mg/kg per day for 21 days (renal dosing adjustment). Succeeding completion of treatment, the patient recovered without neurological sequel and had graft loss.
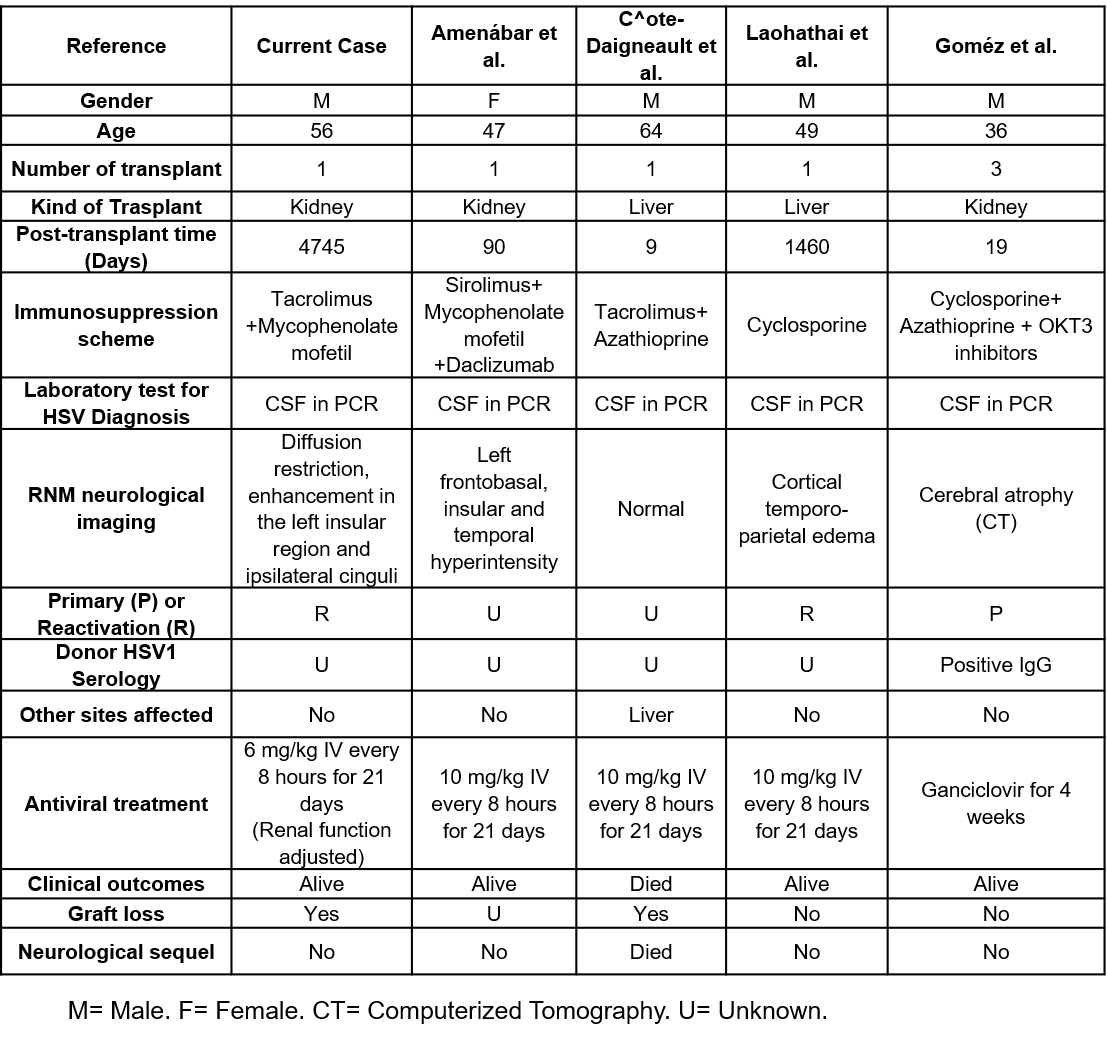
Results and Discussion: We reported a kidney transplant patient who had HSV type 1 encephalitis detected by PCR using CSF, who received standard antiviral treatment and made a recovery without any neurological sequel. Unfortunately, our patient had graft loss. We compared our case report with 4 previous clinical cases already published. We found that these cases had similar outcomes to our case, only 1 case passed away from these cases (Table 1).
Conclusions: We conclude that the early detection and treatment of HSV type I encephalitis could be key for clinical outcomes where opportune prophylaxis could prevent the incidence of this infectious entity.
[1] Lee DH, Zuckerman RA, AST Infectious Diseases Community of Practice. Herpes simplex virus infections in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant [Internet]. 2019 Apr 11 [cited 2019 Apr 29];e13526. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30859647
[2] Gilden DH, Mahalingam R, Cohrs RJ, Tyler KL. Herpesvirus infections of the nervous system. Nat Clin Pract Neurol [Internet]. 2007 Feb [cited 2019 Apr 29];3(2):82–94. Available from: http://www.nature.com/doifinder/10.1038/ncpneuro0401
[3] Netchiporouk E, Tchervenkov J, Paraskevas S, Sasseville D, Billick R. Evaluation of herpes simplex virus infection morbidity and mortality in pancreas and kidney-pancreas transplant recipients. Transplant Proc [Internet]. 2013;45(9):3343–7. Available from: http://dx.doi.org/10.1016/j.transproceed.2013.05.002
[4] Gómez E, Melón S, De Oña M, Alvarez R, Laures A, Alvarez-Grande J. Disseminated herpes simplex virus infection in a renal transplant patient as possible cause of repeated urinary extravasations. Nephron. 1999;82(1):59–64.
[5] Leber A, Everhart K, Demogines A, Fouch S, Barney T, Daly JA, et al. Multi-Center Clinical Evaluation of a Multiplex Meningitis / Encephalitis PCR Panel for Simultaneous Detection of Bacteria , Yeast , and Viruses in Cerebrospinal Fluid Specimens. J Clin Microbiol. 2015;54(9):2251–61.
[6] Ministerio de la Protección Social. Decreto 2493 de 2004. 2004;2004(Agosto 4):1–23. Available from: http://www.ins.gov.co/lineas-de-accion/Red-Nacional-Laboratorios/Marco Legal/Decreto 2493 del 2004.pdf
[7] Amenábar JJ, Durán MI, Montejo M, Lampreabe I. Encefalitis por virus herpes simple en paciente portadora de trasplante renal. Estudio de un caso y revisión de la literatura. Nefrologia. 2006;26(2):270–3.
[8] Côté-Daigneault J, Carrier FM, Toledano K, Wartelle-Bladu C, Willems B. Herpes simplex hepatitis after liver transplantation: case report and literature review. Transpl Infect Dis [Internet]. 2014 Feb [cited 2019 Apr 30];16(1):130–4. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24383552
[9] Laohathai C, Weber DJ, Hayat G, Thomas FP. Chronic herpes simplex type-1 encephalitis with intractable epilepsy in an immunosuppressed patient. Infection. 2016;44(1):121–5.
[10] Gómez E, Melón S, Aguado S, Sánchez JE, Portal C, Fernandez A, et al. Herpes simplex virus encephalitis in a renal transplant patient: diagnosis by polymerase chain reaction detection of HSV DNA. Am J Kidney Dis [Internet]. 1997 Sep [cited 2019 May 3];30(3):423–7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9292572
There are no comments yet...

