
Abdominal aorta calcification prior to kidney transplantation: The association with patient and graft survival
Stan Benjamens1,2, Elsaline Rijkse3, Charlotte A. te Velde-Keyzer4, Derya Yakar2, Martin H. de Borst4, Stefan P. Berger4, Riemer H.J.A. Slart2, Robert C. Minnee3, Robert A. Pol1.
1Division of Transplantation Surgery, Department of Surgery, University Medical Center Groningen, Groningen, Netherlands; 2Medical Imaging Center, University Medical Center Groningen, Groningen, Netherlands; 3Department of Surgery, Erasmus Medical Center, Rotterdam, Netherlands; 4Internal Medicine, University Medical Center Groningen, Groningen, Netherlands
Dutch Kidney Transplant Study Group.
Introduction: A high degree of vascular calcification is commonly encountered in patients undergoing kidney transplantation, especially in those who were on long-term hemodialysis. The prognostic value of pre-transplant vascular calcification for patient and graft survival is unclear. Therefore, this study focused on the association of abdominal aortic calcification (AAC) prior to kidney transplantation and both all-cause mortality and graft failure.
Materials and Methods: From 2005 to 2018, renal transplant recipients referred for a nonenhanced CT procedure within 3 years prior to kidney transplantation, were included in a dual-centre study. Primary endpoints were all-cause mortality and graft failure after kidney transplantation. AAC was retrospectively quantified using a semiautomated tool, as a modified Agatston score. Patients were stratified into three groups based on the AAC quantification results. A Kaplan-Meier curve, with Log Rank analysis, and a Cox proportional hazards model were used for time-to-event analysis. Multivariate analysis included the AAC score in quartiles, recipient age, sex and Body Mass Index (BMI) at moment of transplantation, duration of dialysis prior to transplantation and history of smoking.
Results: We evaluated 547 patients, 461 (84.3%) had detectable calcifications and the median time between CT and transplantation was 1.0 (IQR 0.5 – 1.4) years. Sixty-nine (12.6%) patients died and 84 (15.4%) had graft failure during a median follow-up of 2.5 (IQR 1.0 – 4.3) years. Kaplan-Meier curves indicate that a higher AAC score was associated with a higher all-cause mortality (p < 0.001) (Figure 1.) and higher rate of graft failure (p = 0.009) (Figure 2.). Similarly, in univariate Cox proportional hazard analysis a high AAC score was associated with a higher all-cause mortality (HR 4.3 (95% CI 2.2 – 8.4, p < 0.001) and a higher rate of graft failure (HR 2.1 (95% CI 1.3 – 3.6, p < 0.004). These associations remained significant upon multivariate analysis, with HR 3.1 (95% CI 1.3 – 7.0), p = 0.008) and (HR 2.0 (95% CI 1.2 – 3.5, p < 0.00) for mortality and graft failure, respectively.
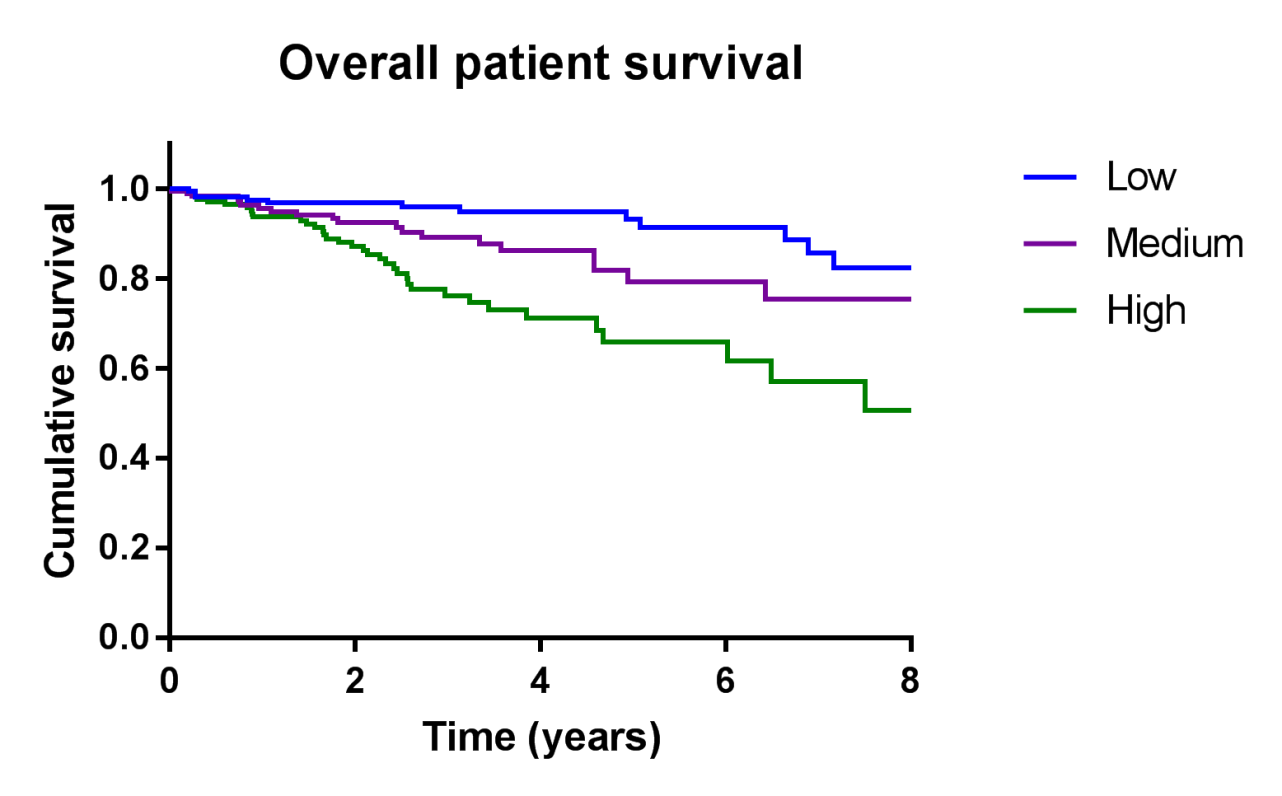
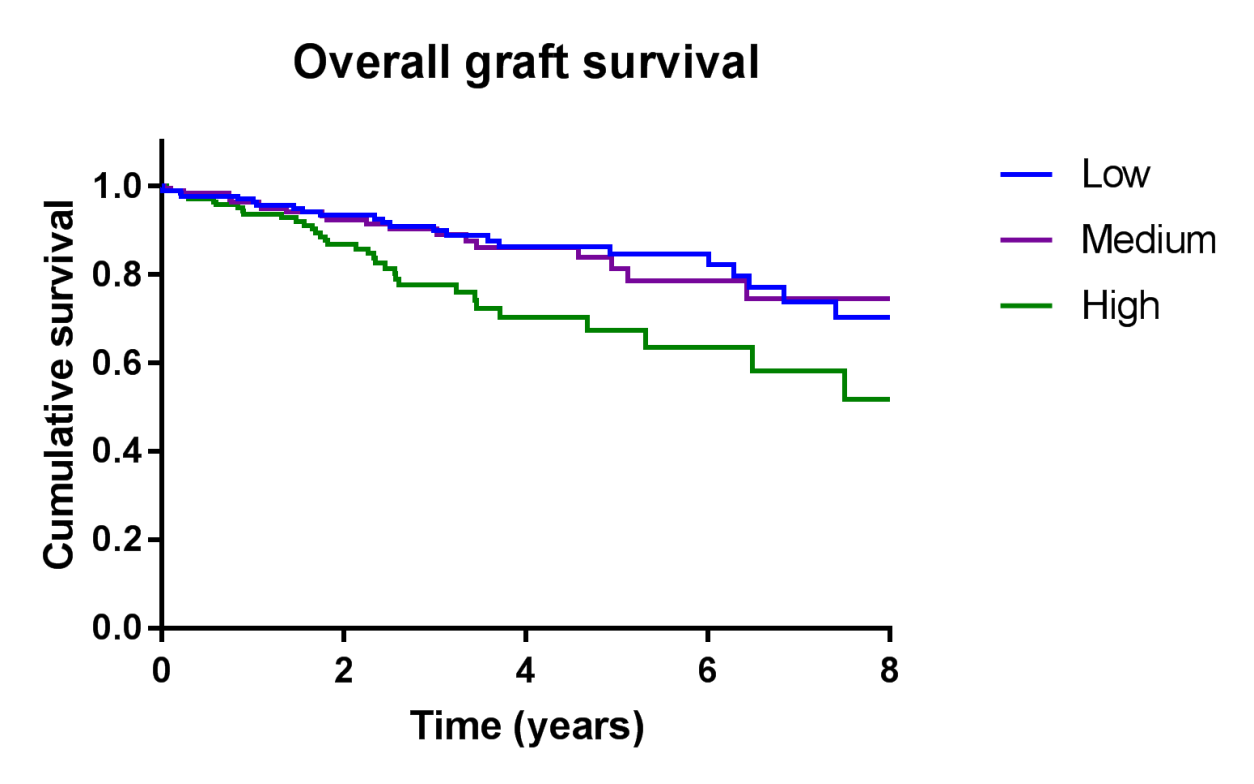
Conclusion: A significant association between the degree of AAC, assessed by nonenhanced CT-based quantification, and both all-cause mortality and graft failure was identified. A validated scoring system for AAC could guide clinicians in decision-making with regard to risk stratification and expected patient-related outcomes after kidney transplantation.
There are no comments yet...